


A 72-year-old woman, with a longstanding history of atrial fibrillation, presented to the dermatology department with a 2-week history of bilateral purpura and leg edema (Figure 1A). She had received a diagnosis of a giant right atrial myxoma 22 years ago, but had refused surgery. Four months prior, she had had a dental procedure, and for the previous 2 months, she had been experiencing general fatigue and weight loss of 6 kg. The patient had been taking apixaban for stroke prevention. We observed red and purple spots on her skin, that were not raised, from the abdomen to the ankles and on both upper arms. On auscultation, systolic and diastolic murmurs were most audible in the second and third right intercostal spaces. Laboratory evaluations showed neutrophil leukocytosis and elevated C-reactive proteins, and cultures from blood samples were positive for Streptococcus mitis. Transesophageal echocardiograms showed a large, pedunculated, calcified myxoma with vegetation, which filled the right atrium and prolapsed into the tricuspid valve orifice during diastole (see Appendices 1 and 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.201351/tab-related-content for video and additional images).
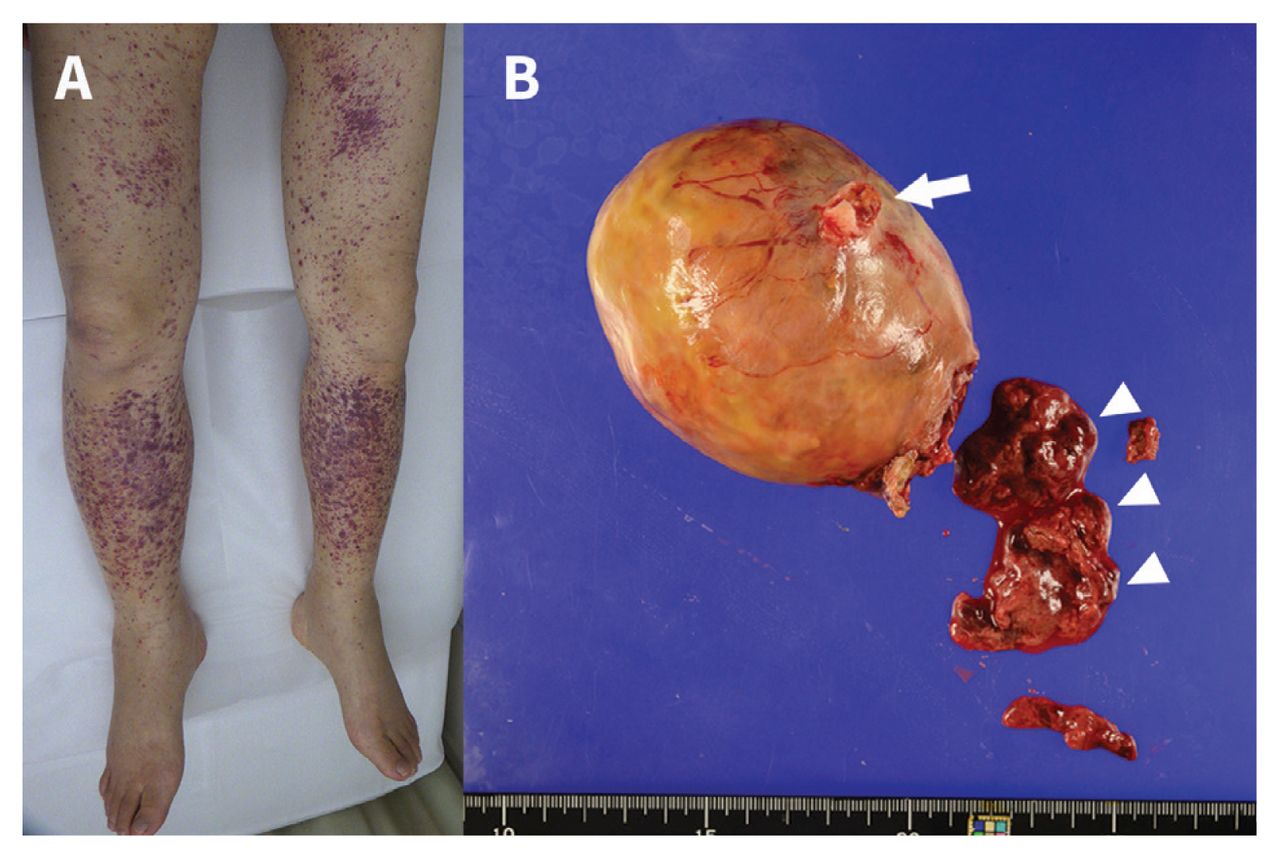
A 72-year-old woman with infection of a calcified myxoma in the right atrium. (A) Photograph showing extensive purpura on the bilateral lower limbs. (B) Photograph showing the excised right atrial myxoma, with red fibrin and vegetation (arrowheads). The atrial attachment site is seen at the surface of the tumour (arrow). The mass measured 8.0 × 8.0 × 8.0 cm.
We diagnosed infective endocarditis related to her pre-existing cardiac myxoma and started antibiotic treatment of intravenous ampicillin (200 mg/kg/d in 4 doses) and gentamicin (3 mg/kg/d in 1 dose). After confirming the susceptibility of the causative organism to penicillin G, we stopped gentamicin after 3 days. Contrast-enhanced computed tomography scans showed 2 small pulmonary infiltrates with central cavitation, consistent with septic pulmonary emboli. Histological examination of the skin showed leukocytoclastic vasculitis. After 5 days of antibiotic treatment, the purpura resolved. The tumour and vegetation (Figure 1B) were resected, and pathological findings were consistent with a degenerative, calcified, cardiac myxoma, with infiltration of neutrophils and bacterial colonies. The patient continued antibiotic therapy for 4 weeks after surgery and recovered without complications.
Approximately 8% of all patients with infective endocarditis develop purpura, and the risk of purpura is related to the size of valvular lesions.1 Many patients with subacute endocarditis have nonspecific symptoms, as this patient did before the development of purpura. Infected cardiac myxoma is exceedingly uncommon. Prompt surgical resection is suggested because of the high risk of embolic events.2 Clinicians should consider infectious endocarditis in patients who develop purpura.
A video of transesophageal echocardiography in a 72-year-old woman with infection of a calcified myxoma in the right atrium is available at Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.201351/tab-related-content
Acknowledgements
The authors thank Dr. Fumito Anno (Department of General Internal Medicine) and Dr. Shu Ichihara (Department of Pathology, National Hospital Organization, Nagoya Medical Center) for useful discussions.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

