


- © 2008 Canadian Medical Association
Worldwide about 1 million people die every year by suicide.1 In Canada an estimated 3665 individuals commit suicide each year, about 500 of whom are 15–24 years old.2 The effects of youth suicide go beyond the victim, affecting the parents, friends and communities of the deceased. Furthermore, youth who survive a suicide attempt continue to be at risk for completed suicide, violent death and poor psychological outcomes. Youth suicide elicits strong reactions from the public, policy-makers and health care providers and has recently been identified as a public health issue by national and provincial initiatives.
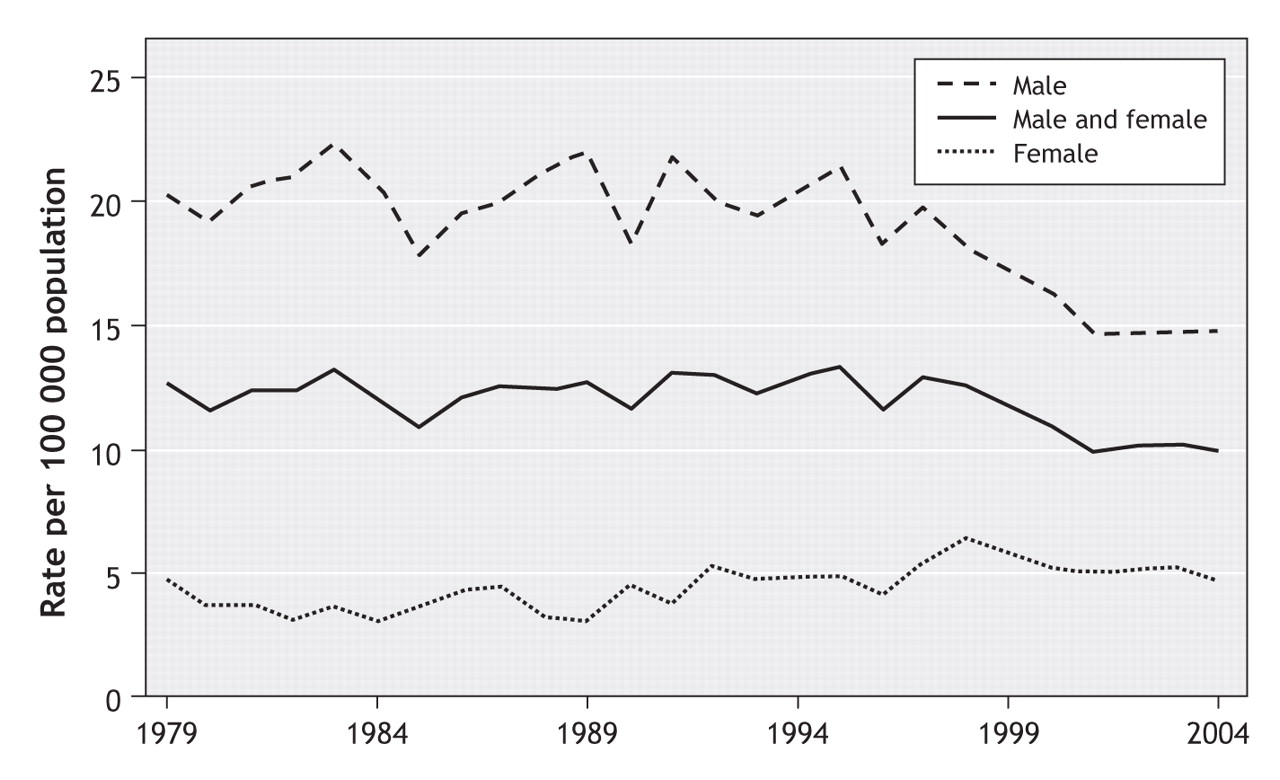
Comparatively, Canadian youth suicide rates, which have decreased in the past decade (Figure 1),2,3 are higher than the rates in the United States,4 Australia5 and the United Kingdom6 (Figure 2) and lower than the rate in New Zealand.7 However, there is substantial variability in regional rates across Canada (Table 1).2 The rate of suicide attempts has remained fairly stable, with youth making up 25% of associated hospital admissions.8 Data comparing rates of completed suicide and suicide attempts suggest that attempts are up to 12 times more common than completed suicides.3 There are sex-related differences in rates, with completed suicides being about 3–5 times more common among males and suicide attempts about twice as common among females.3 Table 2 shows the most common methods of attempted and completed suicide among Canadian youth.
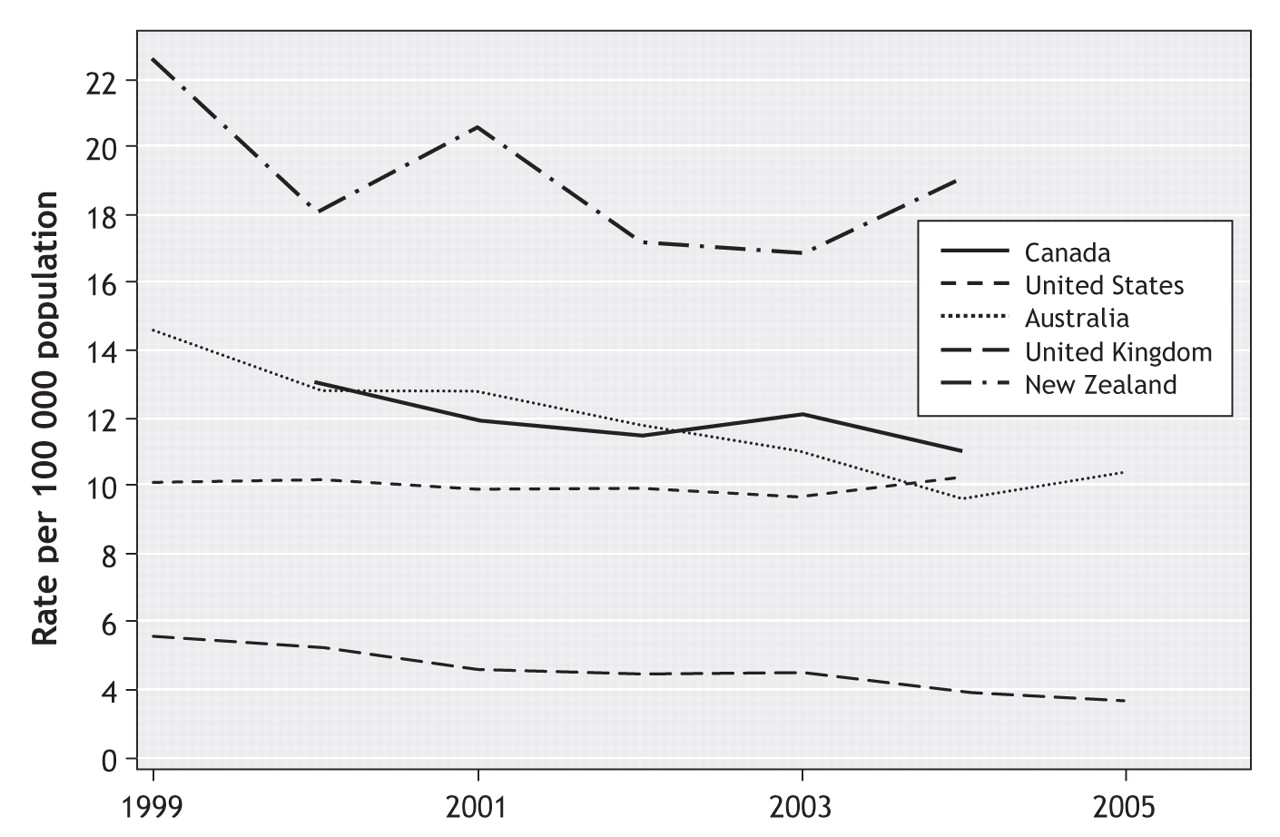
Figure 2: Rates of suicide among people aged 15–24 years in Canada,2 the United States,4 Australia,5 the United Kingdom6 and New Zealand.7 Rates for Canada were calculated as weighted means for the combined age groups 15–19 and 20–24 years. Rates for the United Kingdom were calculated as weighted means for the combined male and female groups.
Table 1.
Table 2.
In general, intentional self-harm and motor vehicle crashes (sometimes also intentional) account for almost 60% of deaths among youth in Canada.9 Although the rate of death from suicide varies across regions of the country, the national rate is about 10 per 100 000 among youth 15–19 years old and 14 per 100 000 among people 20–24 years old.9 Globally, suicide is one of the top 3 causes of death among people 15–34 years old.1 Suicide ranks as an important, potentially preventable cause of death among youth and thus merits substantial public health concern.
Suicide risk factors
Recent systematic reviews have highlighted the current knowledge pertaining to youth suicide.10,11 In Canada, youth who are older, male, Aboriginal or white are more likely to commit suicide than are younger adolescents, children, females and black youth. Besides male sex, characteristics of those who attempt suicide and those who complete it are generally similar.12 Suicide risk factors among Aboriginal youth may differ from those influencing non-Aboriginals; however, substantial scientifically valid data regarding these issues are lacking,13 and there is a great need for rigorous research in this area.
Psychiatric disorders are the most significant risk factor for youth suicide, with over 90% of victims found (sometimes post mortem) to have at least 1 mental health disorder.10 The most common psychiatric diagnoses include affective, conduct and substance use disorders. Multiple psychiatric diagnoses, family history of suicide and previous suicide attempts increase the risk of suicide. Because youth is the life stage associated with onset of major mental health disorders,14 it is not surprising that suicide rates also rise in this age group.
Genetic and neuroendocrine studies have pointed to a number of factors that may be involved in suicidal behaviour independent of the neurobiology of affective disorders. These include low concentrations of serotonin metabolites (e.g., 5-hydroxytryptamine) and variations in genes related to serotonin synthesis (tryptophan hydroxylase), transport (SERT), signaling (HTR1A, HTR2A and HTR1B) and catabolism (MAOA).15 The relative or interactive effects of these factors are not yet understood.
In addition, a number of studies have attempted to link socioeconomic factors and suicide risk. Sexual orientation, social disadvantage, non-intact family of origin, parental history of mental health disorders, family history of suicidal behaviour, personal history of childhood physical or sexual abuse, and dysfunctional parent–child relationship have all been studied as risk factors for youth suicide.10 The causality or effect size of these factors is uncertain.
Other factors include suicide contagion and suicide clusters. The spatial or temporal clustering of suicides is more common among youth than among people in other age groups. Suicide contagion, a term for the spread of suicidal activity usually with reference to media influences, may be associated with sensationalist media reporting of suicide events in the community.10
Interventions
Strategies for suicide prevention frequently focus on risk factors. Ideally these strategies should target risk factors that have been shown to be both causal and modifiable. The scientific evidence for effective interventions is weak, but some strategies show promise.10,11 Much research in this area has suffered from substantial methodological problems, including but not limited to nonrandomization of interventions, the use of surrogate outcome measures, inadequate sample sizes and short duration of evaluation.
Suicide awareness curricula are often used as part of school-based suicide prevention strategies. However, there is little substantial evidence to support their implementation.10 Promising school-based programs include screening students for mental health problems and referring them to mental health professionals and providing teachers with “gatekeeper” training to recognize depression and other mental health disorders in students and to learn the procedures for referral to mental health services. Two other school-based strategies popularly considered to be effective are peer helper programs and postvention (suicide prevention activities, such as crisis debriefing interventions, aimed at youth recently exposed to a suicide). However, these strategies are not supported by sufficient positive evidence to substantiate widespread or unqualified use.16,17
Community-based suicide prevention strategies often target access to methods for self-harm, a known and modifiable risk-factor for suicide. For example, construction of bridge safety barriers, detoxification of cooking gas and car exhaust, changes to packaging of analgesics and restriction of firearms have all been cited as possible prevention strategies.10,11 However, difficulty in measuring direct effects of interventions in the presence of secular trends in suicide rates, coupled with the potential for method substitution, contributes to controversy surrounding the long-term effectiveness of these strategies.
Two other community-based strategies involve the education of media regarding responsible reporting of suicides and the provision of crisis hotlines. Media education programs have been associated with reduced suicide rates in Austria.18 As for crisis hotlines, there is little substantial evidence for their effectiveness in reducing suicide rates.11,19
One promising approach to suicide prevention using the health care system is the training of primary care physicians to recognize, treat and, if necessary, refer patients with mental illness, especially depression.20 Since the treatment of depression has been associated with decreased suicide rates and suicide attempts among youth,21,22 the effective early treatment of depression is an approach that targets a causal as well as a modifiable risk factor. In a national survey about mental health and illness in youth, most of the youth who participated reported that primary care physicians were their first choice for point of contact in case of distress.23 However, in a study assessing the standard of care for pediatric attention-deficit hyperactivity disorder and depression in a region of Ontario, less than 12% of the family physicians surveyed reported comfort in their ability to recognize and treat depression in youth.24 Since training has been found to increase physician identification of suicidal patients25 and to improve treatment of depression and decrease suicide rates,26 it should be more widely available.
A recent clinical report published by the American Academy of Pediatrics Committee on Adolescents underscores the critical role of primary care physicians in the screening, recognition, treatment and referral of youth with mood disorders or suicide risk.27 This document recommends that pediatricians educate themselves and serve as a resource to the community about these issues (Box 1).

Conclusion
Youth suicide is an important public health issue. However, many of the prevention activities currently in place or identified in provincial strategies have not been shown to reduce suicide rates.28 Strategies proven effective in reducing suicide rates, such as early intervention for youth with mental health disorders, are often not available.29 As such, there is a misalignment between the suicide prevention approaches most often implemented and the approaches that have to date been shown to be most effective.
Unless suicide prevention strategies are developed and delivered on the basis of the best available evidence of effectiveness, health providers, parents, educators, politicians and the community may invest in programs that are ineffective or even harmful and deprive youth of programs that could help. The wish to do something should not override our responsibility to do the right thing.
Key points of the article
• Suicide is the second leading cause of death among youth in Canada and one of the top 3 causes of death among youth worldwide.
• The suicide rate among Canadian youth aged 15–19 years is 10.2 per 100 000, with substantial variation across provinces and territories.
• The most substantial risk factors for youth suicide are mental health disorders, family history of suicide and previous suicide attempts.
• Other risk factors include genetic and neuroendocrine factors, socioeconomic factors, and environmental and contextual factors.
• Suggested prevention strategies are often school-based, with others being community- based or involving health care professionals.
• Scientific evidence for effective prevention strategies is weak, but some interventions, such as early identification and effective treatment of mental health disorders in youth, show promise.
• Canada's provinces and territories should implement prevention activities that have the best demonstrated scientific evidence of effectiveness.
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Community-based screening and triage connecting First Nations children and youth to local supports: a cross-sectional study
- Emergency department visits and hospital admissions for suicidal ideation, self-poisoning and self-harm among adolescents in Canada during the COVID-19 pandemic
- Protective and resilience factors to promote mental health among Indigenous youth in Canada: a scoping review protocol
- Peer support for youth suicide prevention: a scoping review protocol
More in this TOC Section
Similar Articles
Collections

