


- © 2008 Canadian Medical Association
The case: A 21-year-old university student presented to hospital with a 1-week history of swelling and discomfort in his right calf. Compression ultrasonography revealed occlusive thrombi in the right superficial femoral and popliteal veins. Investigations, including complete blood count, coagulation studies and renal function tests, yielded normal results. The mean corpuscular volume was elevated (106 fL). Screening for inherited thrombophilia revealed a normal factor V Leiden genotype and factor II variant genotype. Protein C, protein S, antithrombin III and anticardiolipin antibody levels were also normal. The patient was prescribed anticoagulant therapy.
The patient returned 3 months later, reporting progressive gait instability, weakness in both legs and intermittent paresthesia in his feet. He also reported that he was having increasing difficulty concentrating on his university courses and that his marks had slipped. Findings on physical examination were consistent with cobalamin (vitamin B12) deficiency (Table 1). The hemoglobin concentration was 139 g/L, and the mean corpuscular volume was 108 fL. The leukocyte and platelet counts were normal. A peripheral blood smear showed round macrocytes. The serum cobalamin level was decreased (55 pmol/L), and the plasma homocysteine level was elevated (88 μmol/L). The red blood cell folate level was normal, and results of the Schilling test and a test for anti-intrinsic factor antibodies were negative.
Table 1.
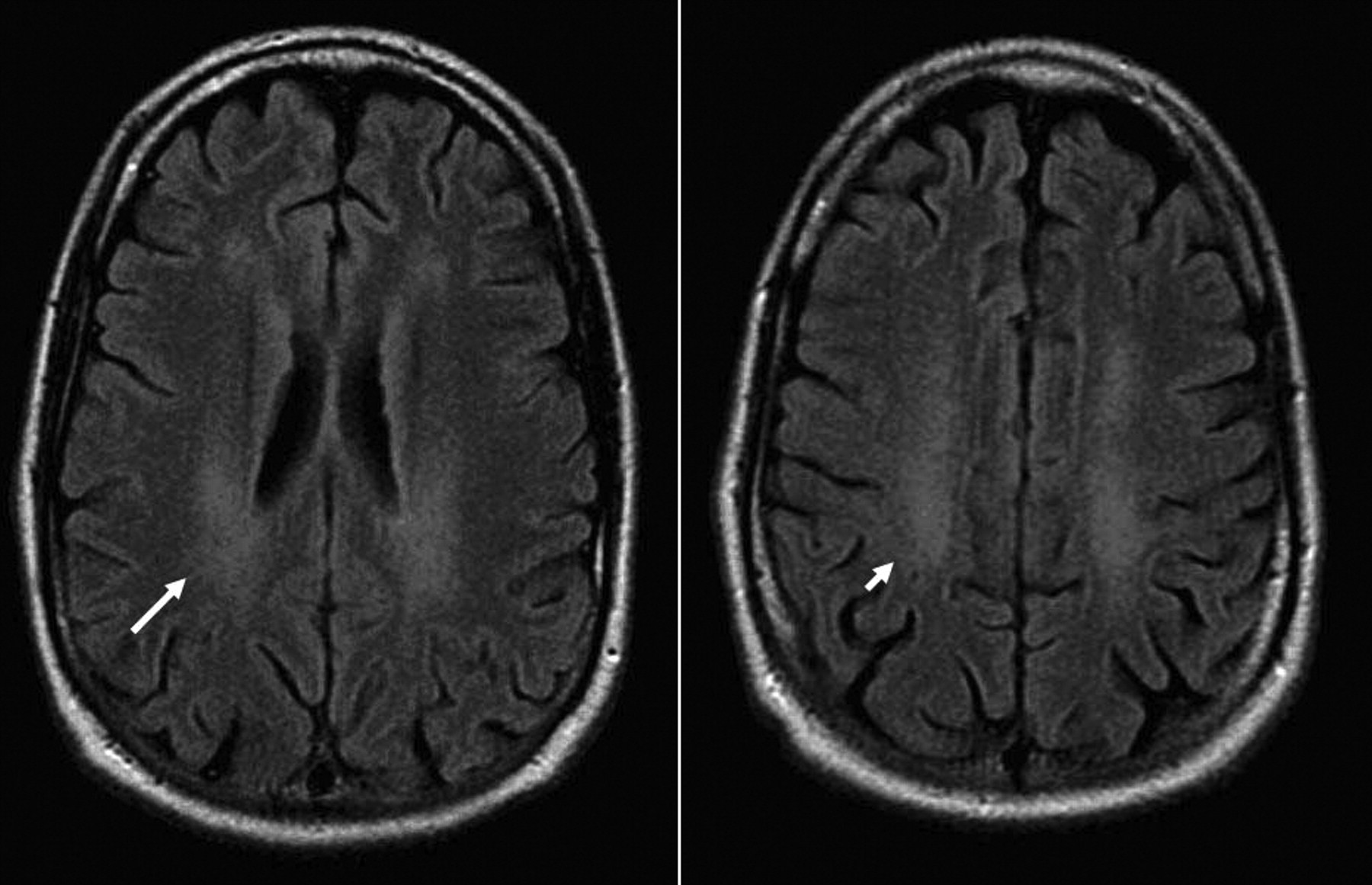
Magnetic resonance imaging of the brain revealed atrophic changes, and fluid-attenuated inversion recovery (FLAIR) sequences showed diffuse hyperintense signal changes in the periventricular and deep subcortical white matter involving both hemispheres (Figure 1). Magnetic resonance imaging scans of the spine were unremarkable.

Figure 1: Magnetic resonance imaging scans of the brain, showing changes consistent with cobalamin deficiency. Fluid-attenuated inversion recovery (FLAIR) images show diffuse hyperintense signal changes in the periventricular (long arrow) and deep subcortical white matter (short arrow) involving both cerebral hemispheres. Moderate atrophy is demonstrated by sulcal widening to an extent not in keeping with the patient's age.
Further history revealed that the patient's diet was limited to toasted oats cereal (Cheerios) without milk and to bread and french-fried potatoes. The patient admitted to a profound aversion to most foods and textures, including meat, and avoided all but a limited diet since early childhood. There were no elements suggestive of a mood, anxiety or eating disorder.
The patient was given cobalamin injections daily for 1 week, followed by weekly injections for 1 month and then monthly injections. The anticoagulation therapy was continued. Eight weeks later, he reported improvement in his gait, mood and academic performance. His motor power had increased, but his reflex and sensory abnormalites persisted. At follow-up 2 years later, all neurologic deficits had resolved. Despite psychological intervention, however, he continued to avoid most foods. He successfully completed his university degree and is now working full-time.
Cobalamin plays a vital role in the synthesis of DNA. Severe cobalamin deficiency manifests clinically as a syndrome involving either or both the neurologic and hematopoietic systems (Box 1). Although cobalamin deficiency usually presents with anemia or macrocytosis, neurologic manifestations may sometimes precede the hematologic disorder. In a series of 141 consecutive patients with neuropsychiatric abnormalities due to cobalamin deficiency, Lindenbaum and colleagues1 found that 28% had neither anemia nor macrocytosis.1 These observations suggest that the absence of macrocytosis or anemia does not exclude a diagnosis of cobalamin deficiency.

Serum levels of homocysteine are elevated in patients with cobalamin deficiency, owing to cobalamin's role in homocysteine metabolism (Figure 2), and usually return to normal with vitamin replacement. In their series of 141 patients, Lindenbaum and colleagues1 noted that 36 of the 37 patients who had their homocysteine level measured had a level above 3 standard deviations from the mean for normal controls.1 Hyperhomocysteinemia on its own is associated with an increased risk of myocardial infarction, stroke and venous thrombosis.2 However, it is unclear whether the hyperhomocysteinemia in patients with cobalamin deficiency also promotes such thrombotic complications.3 Our patient had no apparent risk factors for venous thrombosis other than the hyperhomocysteneimia associated with cobalamin deficiency. There is insufficient evidence to recommend cobalamin testing in patients with idiopathic deep vein thrombosis. An oral dose of 1000 or 2000 μg of cobalamin, initially taken daily and thereafter weekly and then monthly, may be as effective as intramuscular administration in obtaining short-term hematologic and neurologic responses in patients with cobalamin deficiency.4

Figure 2: The role of cobalamin in homocysteine metabolism. Methylcobalamin is a cofactor in the synthesis of methionine from homocysteine. Cobalamin deficiency is characterized by elevations in serum homocysteine levels.
Diets of most adults in North America provide the recommended intake of cobalamin, since it is readily found in animal foods, dairy products, eggs and fortified breakfast cereals. One serving of Cheerios, a major component of our patient's diet, contains 25% of the recommended daily allowance if purchased in the United States (www.cheerios.com/ourCereals/Cheerios/Cheerios_home.aspx) and 75% if purchased in the United Kingdom (www.cpuk.co.uk/brands/cheerios.aspx). The recommended daily allowance for cobalamin is 2.4 μg in Canada and the United States, and 1.5 μg in the United Kingdom. Our patient consumed Cheerios purchased in Canada, which does not contain cobalamin (www.cheerios.ca/en/nutrition.html), since its addition to breakfast cereals is currently prohibited under section B.13.060 of the Food and Drug Regulations. A revised policy — whereby the addition of 0.4–2.4 μg per reference amount will be permitted at the discretion of manufacturers — is expected to be implemented through regulatory proposals published in the Canada Gazette Part I for comment in the near future.5 Interestingly, if our patient had lived in the United States or the United Kingdom, his dietary habits may not have resulted in cobalamin deficiency.
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

