


Abstract
Background: When patients and physicians speak the same language, it may improve the quality and safety of care delivered. We sought to determine whether patient–physician language concordance is associated with in-hospital and postdischarge outcomes among home care recipients who were admitted to hospital.
Methods: We conducted a population-based study of a retrospective cohort of 189 690 home care recipients who were admitted to hospital in Ontario, Canada, between 2010 and 2018. We defined patient language (obtained from home care assessments) as English (Anglophone), French (Francophone) or other (allophone). We obtained physician language from the College of Physicians and Surgeons of Ontario. We defined hospital admissions as language concordant when patients received more than 50% of their care from physicians who spoke the patients’ primary language. We identified in-hospital (adverse events, length of stay, death) and post-discharge outcomes (emergency department visits, readmissions, death within 30 days of discharge). We used regression analyses to estimate the adjusted rate of mean and the adjusted odds ratio (OR) of each outcome, stratified by patient language, to assess the impact of language-concordant care within each linguistic group.
Results: Allophone patients who received language-concordant care had lower risk of adverse events (adjusted OR 0.25, 95% confidence interval [CI] 0.15–0.43) and in-hospital death (adjusted OR 0.44, 95% CI 0.29–0.66), as well as shorter stays in hospital (adjusted rate of mean 0.74, 95% CI 0.66–0.83) than allophone patients who received language-discordant care. Results were similar for Francophone patients, although the magnitude of the effect was smaller than for allophone patients. Language concordance or discordance of the hospital admission was not associated with significant differences in postdischarge outcomes.
Interpretation: Patients who received most of their care from physicians who spoke the patients’ primary language had better in-hospital outcomes, suggesting that disparities across linguistic groups could be mitigated by providing patients with language-concordant care.
A growing number of people in Canada (more than 6.1 million in 2016) are faced with the challenge of living in a situation in which their primary language is not spoken by most of the population and is not recognized as an official provincial or territorial language. 1,2 We refer to this as a minority language situation, and such people include Francophones living outside of Quebec, Anglophones living in Quebec, and all residents of Canada whose primary language is a language other than English or French (allophones). Numerous studies have shown that people in North America with limited English proficiency generally have poorer access to health care and receive health care services of lower quality and safety, resulting in higher risk of adverse events and increased health resource use.3–8 Despite these findings, few authors have considered the impact of patient–provider language concordance, whereby patients and providers have proficiency in a shared language.9 Studies in the United States have shown that patients with asthma who receive language-concordant primary care are less likely to omit medications, miss appointments or visit the emergency department.10 Patients with diabetes who receive language-concordant care have improved glycemic and low-density-lipoprotein control,11,12 as well as increased participation in diabetic foot care programs.13 Although patient language is generally considered to be a nonmodifiable risk factor, language discordance represents a potentially modifiable variable, which could be the target of interventions (e.g., by referring patients to providers who have proficiency in their primary language).
Frail patients are more likely to have communication problems and poor health outcomes than the general population; thus, language concordance may be particularly important in this patient population.14,15 The risk of harm for frail, older patients has been attributed to medical complexity and multi-morbidity; 16–18 however, since communication barriers also increase with age, older patients may also be more likely to experience harm because of poor patient–provider communication. 19 Most studies of language concordance have been limited to the primary care setting. We are aware of 2 studies conducted in the acute care setting, with 1 showing that Francophones residing in Ontario were less likely to experience harm when they were treated in hospitals that were required by law to provide services French. 20,21
We sought to compare the risk of adverse, hospital-related outcomes among frail patients living in Ontario, Canada, after stratifying by patient language and patient–physician language concordance or discordance. We hypothesized that patients receiving language-concordant care would have better outcomes than those receiving language-discordant care.
Methods
Setting
Canada has a population of about 36 million people, of which 58.1% and 21.5% report English or French, respectively, as their primary language.2 Since the Official Languages Act of 1969, both English and French have been recognized as official languages at the federal level.22 However, only 1 province (New Brunswick) recognizes both English and French as official languages; the remaining provinces and territories are unilingual. As a result, considerable linguistic heterogeneity exists across Canada. Linguistic diversity is especially pronounced in Ontario (Canada’s most populous province), where 33.1% of the population report a primary language other than English, which is the province’s only official language.2 Although French is not recognized as an official language in Ontario, the French Language Services Act requires a small number of government agencies to provide all of their services in both English and French; this includes 12 hospitals, of which 4 are in the Champlain region and 8 are in Northern Ontario.23
Study design and population
We conducted a population-based, retrospective cohort study in Ontario, Canada. Our baseline cohort consisted of all residents receiving publicly funded, long-term, home care services from Apr. 1, 2010, to Mar. 31, 2018, with 2 or more comorbidities who were admitted to hospital within 1 year of their first home care assessment (index assessment). We excluded residents who were younger than 18 years or older than 105 years at the index assessment, those who were not eligible for the Ontario Health Insurance Plan (OHIP) at any time during the study window and those who were missing data for age or sex. Among this cohort, we identified patients with an index hospital admission during the study window.
Data sources
We used administrative databases at ICES, an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. We linked the Resident Assessment Instrument–Home Care (RAI-HC), which is a standardized data collection form for publicly funded home care assessments that includes the language of the patient,24 to numerous administrative databases using anonymized, unique encoded identifiers. The College of Physicians and Surgeons of Ontario (CPSO) maintains a database with demographic information on all physicians in Ontario, and the OHIP database records all physician billing claims. The Discharge Abstract Database and the National Ambulatory Care Reporting System provide data on admissions to acute care treatment facilities and ambulatory care visits, respectively. The Immigration, Refugees and Citizenship Canada (IRCC) Permanent Resident Database identifies immigrants who were granted citizenship or permanent residency after 1985.25 Finally, the Registered Persons Database provides Ontario residents’ age, sex and postal code. We linked each resident’s postal code to the 2016 Statistics Canada Census to obtain neighbourhood income quintile and urban or rural status. We ascertained chronic conditions using algorithms validated by ICES and applied in previous studies (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.212155/tab-related-content).
Exposure
We obtained patient language from the RAI-HC database. During these assessments, interviewers determine the home care recipient’s primary language by listening, observing and, if necessary, asking the home care recipient to specify their primary language. We previously validated this language variable by comparing it to self-reported language obtained from the Canadian Community Health Survey; we assessed agreement using Cohen κ,26 which we found to be substantial (κ = 0.76) (Batista and colleagues, Institut du Savoir Monfort: unpublished data, 2020).
We defined Anglophones and Francophones as residents whose primary language was English and French, respectively. The remaining languages were combined to form groups of mutually understandable languages (i.e., languages that are different from one’s language but still readily understood without prior familiarity or special effort).27–29 We retained the 10 most commonly spoken language groups in our cohort. We defined allophones as residents whose primary language was included in 1 of these 10 groups.
Next, we obtained physician language from the CPSO database. All physicians in Ontario are invited to submit the languages that they speak at the time of registration with CPSO. We identified physicians who self-identified as speaking English, French or any of the 10 groups of allophone languages that we identified among our cohort of patients. Since all physicians in Ontario are required to speak English, Anglophone patients were considered to have been treated in a language-concordant setting. A complete description of the classification of both patient and physician languages is presented in Appendix 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.212155/tab-related-content.
For each index hospital admission, we identified all physicians who provided care during the admission using billing data in the OHIP database. We defined physician care as language concordant if both the patient and the physician shared a mutually intelligible language,27–29 and defined all other physician care as language discordant. We then determined language concordance of the entire admission by calculating a weighted average of all physician care, taking into consideration the number of days of care provided by each physician from admission to discharge. In other words, for each patient, we took the sum of the number of days of care provided by physicians who spoke their primary language, and we divided this by the total number of days of care provided by all physicians (irrespective of language). Thus, physicians who provided care for a greater number of days had a relatively larger impact on the language concordance status. Patients who received more than 50% of their care from physicians who spoke a language that was mutually intelligible to their primary language were deemed to have been treated in a language-concordant setting; all other patients were considered to have been treated in a language-discordant setting. We excluded admissions if physician language was missing for more than 50% of days billed by physicians.
Outcomes
We considered both in-hospital and postdischarge outcomes. In-hospital outcomes included adverse events, length of stay (number of days from admission to discharge) and death. We identified adverse events using the patient safety indicators developed by Southern and colleagues (details included in Appendix 3, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.212155/tab-related-content).30 In this study, we defined a harmful hospital admission as an admission with at least 1 diagnosis code relating to an adverse event, as defined in the patient safety indicators. Postdischarge outcomes included emergency department visits, readmissions to hospital and death occurring within 30 days of discharge (among patients who were discharged alive).
Statistical analysis
We performed descriptive analyses to compare patient characteristics and outcomes across linguistic groups and after stratifying by patient–provider language concordance or discordance. We determined the effect of language concordance or discordance using logistic regression for binary variables, and using negative binomial regression for length of stay. We used separate models to determine the impact of language concordance or discordance among Francophones and allophones. Patients receiving care in language-discordant settings were the reference group in all analyses. Adjusted analyses included the potential confounders of age at admission, sex, marital status, education, income quintile, geographic region, urban or rural residence, immigration status, Charlson Comorbidity Index,31 Diagnostic Risk Score,32 activities of daily living (ADL) scale,33 instrumental ADL scale,34 cognitive performance scale35 and changes in health, end-stage disease, signs and symptoms (CHESS) score.36 Statistical tests were 2-tailed and the significance threshold was set at 0.05.
Sensitivity analysis
Since the rate of in-hospital death can affect the average length of stay in hospital, we performed sensitivity analyses by repeating analyses for length of stay after removing all hospital admissions that ended in death.
Ethics approval
The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board.
Results
The initial cohort that met eligibility criteria included 248 311 home care recipients. Among allophones, we retained the 10 most commonly spoken language groups in our cohort, including Italian (n = 8361), Mandarin (n = 3426), Ibero-Romance (n = 3162), Indo-Aryan (n = 2286), West Slavic (n = 1567), West Germanic (n = 1471), East Slavic (n = 1425), Greek (n = 1264), Dravidian (n = 1073) and Arabic (n = 916), resulting in exclusion of 21.3% of allophones. After excluding the recipients whose language was not included, those missing data on language and those missing physician language, our final cohort included 189 690 home care recipients (Figure 1). Of these, 71 913 (37.9%) had multiple hospital admissions during the study window.

Study flow diagram. Note: RAI-HC = Resident Assessment Instrument–Home Care, OHIP = Ontario Health Insurance Plan.
Table 1 presents the baseline characteristics of the cohort. Most home care recipients were Anglophone (84.1%), and Francophones and allophones represented 2.7% and 13.2% of the cohort, respectively. Compared with Anglophones, Francophones and allophones were generally older and less likely to have completed high school. Francophones were most likely to live in rural areas and reside in lower-income neighbourhoods. Allophones were most likely to have immigrated to Canada.
Baseline characteristics of home care recipients
The functional status and health characteristics of the cohort are presented in Table 2. The burden of chronic multimorbidity was similar across linguistic groups. However, both Francophones and allophones had more cognitive impairment than Anglophones. Compared with Anglophones, allophones were more likely to have functional limitations and Francophones were more likely to have greater health declines, denoted by higher CHESS score.
Health characteristics and functional status of home care recipients
Physician language was missing for 13 251 physicians (24.3%), which resulted in the exclusion of 50 336 hospital admissions (21.0%) where more than 50% of days billed by physicians were missing language data. Slightly more than half of physicians (58.3%) were Anglophone, and the remainder of physicians (41.7%) were multilingual. Almost half of Francophone patients (44.4%) were treated primarily by French-speaking physicians. Only 1.6% of allophones received most of their care from physicians who spoke a language that was mutually intelligible to their primary language.
Outcomes
In the adjusted regression analyses, allophones who were treated in language-concordant settings had lower risk of adverse events during hospital admission (adjusted odds ratio [OR] 0.26, 95% confidence interval [CI] 0.15–0.44), shorter stays in hospital (adjusted rate of mean 0.77, 95% CI 0.68–0.86), and lower risk of in-hospital death (adjusted OR 0.46, 95% CI 0.31–0.70) than allophones who received language-discordant care (Figure 2). Similarly, Francophones who received language-concordant care were significantly less likely to have a harmful hospital admission (adjusted OR 0.64, 95% CI 0.52–0.77) or die in hospital (adjusted OR 0.76, 95% CI 0.62–0.95) than Francophones who received language-discordant care. Furthermore, the average length of stay in hospital was 7% shorter for Francophones who received language-concordant care (adjusted rate of mean 0.93, 95% CI 0.87–1.00).
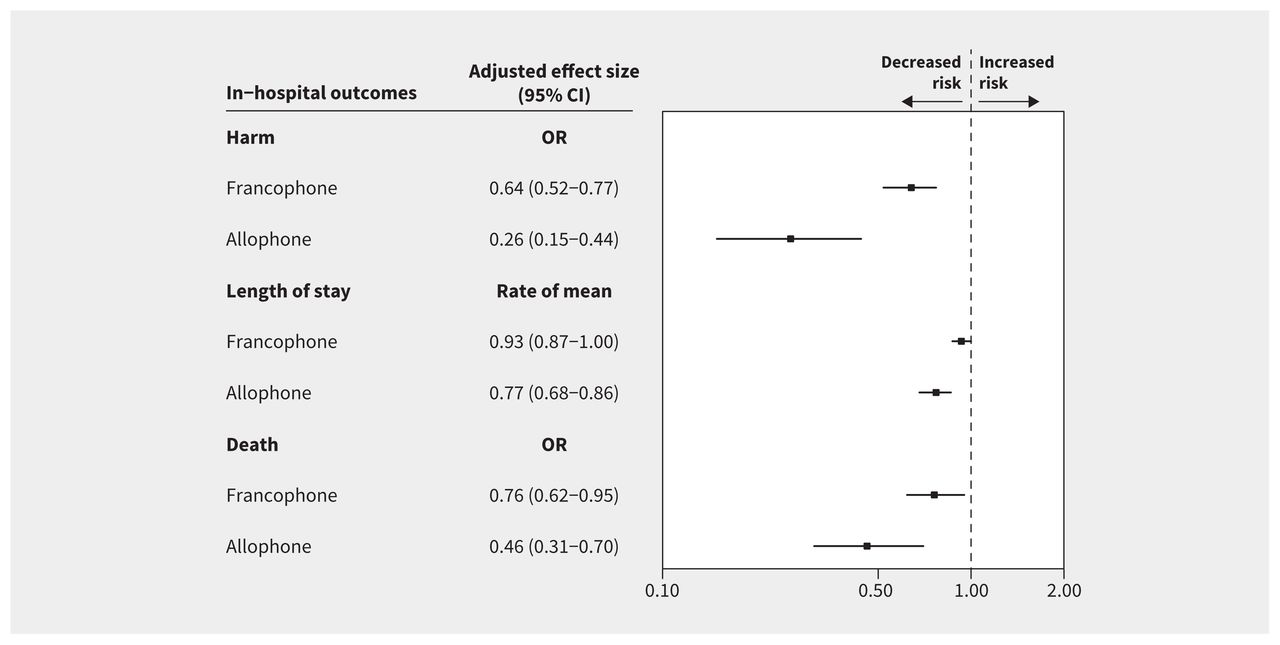
Adjusted in-hospital outcomes for Francophone and allophone recipients of home care. Language-discordant care is the reference in all analyses. Values to the left of the line of null effect denote lower risk of harm (i.e., record of 1 or more adverse events during hospital admission), shorter stays in hospital and lower risk of death among patients receiving language-concordant care; values to the right of the line of null effect denote higher risk of harm, longer stays in hospital and higher risk of death among patients receiving language-concordant care. Effect sizes adjusted for age at admission, sex, marital status, education, income quintile, geographic region, urban or rural residence, immigration status, Charlson Comorbidity Index, diagnostic risk score, activities of daily living (ADL) scale, instrumental ADL scale, cognitive performance scale and changes in health, end-stage disease, signs and symptoms (CHESS) score. Note: CI = confidence interval, OR = odds ratio.
Of the 189 690 patients included in this study, 165 549 (87.3%) were discharged alive. The rates of return emergency department visits, readmissions to hospital and death within 30 days of discharge were not significantly different when comparing both Francophone and allophone patients who received language-concordant care to their counterparts who received language-discordant care (Figure 3).
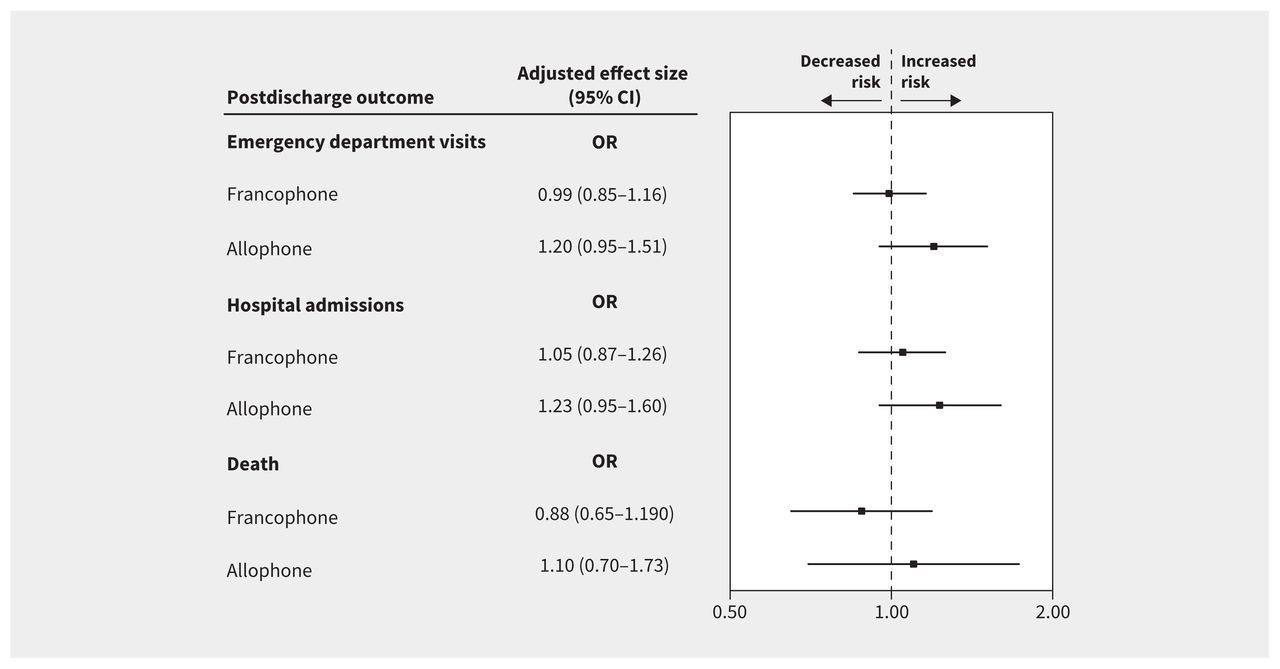
Adjusted postdischarge (within 30 days of discharge) outcomes for Francophone and allophone recipients of home care. Language-discordant care is the reference in all analyses. Values to the left of the line of null effect denote lower risk of emergency department visits, hospital admissions and death among patients receiving language-concordant care; values to the right of the line of null effect denote higher risk of emergency department visits, hospital admissions and death among patients receiving language-concordant care. Effect sizes adjusted for age at admission, sex, marital status, education, income quintile, geographic region, urban or rural residence, immigration status, Charlson Comorbidity Index, diagnostic risk score, activities of daily living (ADL) scale, instrumental ADL scale, cognitive performance scale and changes in health, end-stage disease, signs and symptoms (CHESS) score. Note: CI = confidence interval, OR = odds ratio.
Complete regression models for in-hospital and postdischarge outcomes are presented in Appendix 4 and Appendix 5, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.212155/tab-related-content, respectively. Sensitivity analyses for length of stay are presented in Appendix 6, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.212155/tab-related-content.
Interpretation
In this study of home care recipients admitted to hospital in Ontario, Canada, we found that Francophones and allophones who received language-concordant physician care were less likely to have adverse events, more likely to have shorter hospital stays and less likely to die in hospital when compared with their counterparts who received language-discordant care. However, language concordance was not associated with significant differences in postdischarge outcomes (emergency department visits, readmissions to hospital and death within 30 days of discharge).
The lower risks of adverse events and in-hospital death observed among patients receiving language-concordant care may partially be explained by enhanced patient–provider communication (e.g., ability to elicit symptoms and obtain a complete medical history), which can improve the accuracy and timeliness of diagnoses made by physicians.37,38 Physicians who cannot effectively communicate with their patients are more likely to perform additional (and sometimes unnecessary) investigations, 39,40 which could result in an increased risk of adverse events and prolonged stays in hospital. Clear and effective patient–provider communication also has the potential to improve patient cooperation and engagement, which is associated with positive health outcomes.41 Lastly, the results of our study may be influenced by patient–provider cultural differences, which correlate with linguistic discordance and have been shown to have a negative impact on patient care.42
The benefits of receiving language-concordant care were more pronounced for allophones than Francophones. This finding may be explained by higher rates of bilingualism among Francophone patients. According to the 2016 Canadian Census, 93% of Franco-Ontarians report being able to conduct a conversation in English.2 A previous study of home care recipients in Ontario also found that 7.7% of Francophones had low English proficiency, compared with 52.9% of allophones.8 It is likely that fewer Francophone patients receiving language-discordant care had a severe language barrier when interacting with physicians, all of whom reported being able to speak English. Furthermore, although French is not recognized as an official language in Ontario, provincial legislation requires the provision of services in French in certain regions (e.g., Eastern and Northern Ontario).43 Thus, some Francophone patients may have benefited from receiving language-concordant care in these hospitals (e.g., from nursing staff, personal support workers) despite being treated by Anglophone physicians.
Previous studies have shown that patients who face language barriers have an increased risk of return emergency department visits or readmissions to hospital.44–48 These findings have been attributed to poor understanding of discharge instructions, as well as to the quality of care received during the hospital admission.47,49 Most studies on this topic have focused on younger populations in the United States or patients with specific chronic conditions.44–48 We focused on older patients with chronic multimorbidity, but we did not observe significant differences for any of the postdischarge outcomes between patients who received language-concordant or language-discordant care. This may be driven, at least in part, by cultural differences in preference for community-based care over hospital-based care,50 a finding that we previously reported among frail patients receiving home care services in Ontario.51 Furthermore, the null findings may be owing to the complex and multifactorial nature of health care use among older patients, which is influenced by factors such as the patient’s goals of care, functional and health status at discharge, and level of support at home.52–54
Limitations
We obtained patient language and information related to functional status from home care assessments. Previous analyses conducted by our group showed substantial agreement (κ = 0.76) between the language variable obtained from home care assessment and that obtained from the Canadian Community Health Survey (Batista and colleagues, Institut du Savoir Monfort: unpublished data, 2020). However, since only 1 language can be recorded during these assessments, we may have overestimated language discordance, especially for multilingual residents whose primary language is not English, but who may be fluent in English. Such misclassification would lead to patients being incorrectly identified as having had a language-discordant hospital admission, which would bias the results toward the null. The quality of data collected in the RAI-HC may be affected by language concordance or discordance of the assessment, as interviewers (predominantly Anglophone) may encounter language barriers when trying to elicit information from Francophones and allophones. Furthermore, the measures used to estimate functional status in the RAI-HC (e.g., ADL scale, instrumental ADL scale, cognitive performance scale) have not been validated among Francophone and allophone populations.
To identify patients who received most of their care in a language-concordant setting, we calculated a weighted average of the number of days where patients received care from physicians who spoke their primary language. As we do not have information regarding the duration or the nature of patient–physician interactions, our analysis assumes that all patient–physician interactions had an equal impact on patient outcomes. Furthermore, the physician language variable in CPSO has not been validated; as such, the results may be subject to misclassification. Since language is recorded independently from patient outcomes, misclassification should be non-differential, leading the results to be biased toward the null. Patients interact with many health care providers, some of whom are likely to speak several languages, and thus may be able to provide translation for other members of the health care team. It was also not possible to determine whether patients and their health care providers communicated in a mutually intelligible language or whether interpreter services were used. Finally, since Anglophones, Francophones and allophones in our cohort differed significantly with regard to age, socioeconomic status and urban or rural residence, as well as health characteristics and functional status, the possibility of residual confounding remains.
Conclusion
Francophone and Allophone recipients of home care who received language-concordant care during their hospital admission had better in-hospital outcomes than their counterparts who received language-discordant care. The results persisted after adjusting for potentially confounding variables, suggesting that the findings can be attributed to linguistic factors rather than differences in patient characteristics. Hospital administrators should identify patients living in minority language situations and consider implementing measures to increase the provision of language-concordant care to these patients (e.g., by referring patients to physicians who have proficiency in a shared language).
Footnotes
Competing interests: Claire Kendall reports support from the Canadian Institutes of Health Research and the University of Ottawa Faculty of Medicine. Manish Sood reports speaker fees from AstraZeneca. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Emily Seale, Michael Reaume, Ricardo Batista, Anan Bader Eddeen and Peter Tanuseputro contributed to the conception of the work. Emily Seale, Michael Reaume, Ricardo Batista, Anan Bader Eddeen, Rhiannon Roberts, Emily Rhodes, Daniel McIsaac, Claire Kendall, Manish Sood, Denis Prud’homme and Peter Tanuseputro contributed to the study design. Rhiannon Roberts and Emily Rhodes facilitated data acquisition. Emily Seale, Michael Reaume and Anan Bader Eddeen performed data analyses. Emily Seale, Michael Reaume, Anan Bader and Peter Tanuseputro interpreted the data. Emily Seale, Michael Reaume, Ricardo Batista, Anan Bader Eddeen, Rhiannon Roberts, Emily Rhodes, Daniel McIsaac, Claire Kendall, Manish Sood, Denis Prud’homme and Peter Tanuseputro drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding: This study was primarily supported by Institut du Savoir Montfort and the Programme de subventions Savoir Montfort (concours 2018–2019), funded by Fondation Montfort. The study was also supported by the Bruyère Centre for Individualized Health.
Data sharing: The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by Ontario Ministry of Health (MOH). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. Parts or whole of this material are based on data and/or information compiled and provided by Immigration, Refugees and Citizenship Canada (IRCC), current to 2018. However, the analyses, conclusions, opinions and statements expressed in the material are those of the authors, and not necessarily those of the IRCC. Parts of this material are based on data or information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed in the material are those of the authors, and not necessarily those of CIHI. This study uses data adapted from Statistics Canada, Census Profile, 2016. This does not constitute an endorsement by Statistics Canada of this product.
- Accepted June 8, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article extras
Article tools



Jump to section
Related Articles
Cited By...
- Understanding linguistic inequities in healthcare: moving from the technical to the social
- Association between language discordance and unplanned hospital readmissions or emergency department revisits: a systematic review and meta-analysis
- Applying an equity lens to hospital safety monitoring: a critical interpretive synthesis protocol
- Distance, access and equity: a cross-sectional geospatial analysis of disparities in access to primary care for French-only speakers in Ottawa, Ontario
More in this TOC Section
Similar Articles
Collections

