


Article Figures & Tables
Figures
- Figure 1:
Nomogram for designation of risk among 2840 well newborns at ≥ 36 weeks’ gestation and birth weight ≥ 2000 g, or at ≥ 35 weeks’ gestation and birth weight ≥ 2500 g, based on the hour-specific serum bilirubin values. The serum bilirubin level was obtained before discharge, and the zone in which the value fell predicted the likelihood of a subsequent bilirubin level exceeding the 95th percentile. Because of sampling bias, this nomogram should not be used to represent the natural history of neonatal hyperbilirubinemia. Reproduced with permission from the American Academy of Pediatrics guidelines, (3) Pediatrics 2004;114:297–316. Copyright © 2004 American Academy of Pediatrics.
- Figure 2:
Algorithm providing recommendations for management and follow-up according to predischarge bilirubin measurements, gestational age and risk factors for subsequent hyperbilirubinemia. G6PD = glucose-6-phosphate dehydrogenase.
Provide lactation evaluation and support for all breastfeeding mothers.
Recommendation for timing of repeat total serum bilirubin (TSB) or transcutaneous bilirubin (TcB) measurement depends on infant’s age at measurement and how far the level is above the 95th percentile (Figure 1); higher and earlier initial levels require an earlier repeat measurement.
Perform standard clinical evaluation at all follow-up visits.
For evaluation of jaundice, see the 2004 American Academy of Pediatrics guideline. (3)
Reproduced with permission from Maisels et al., (5) Pediatrics 2009;124:1193–8. Copyright © 2009 American Academy of Pediatrics.
- Figure 3:
Probability of severe hyperbilirubinemia developing based on a newborn’s predischarge bilirubin level and gestational age. Severe hyperbilirubinemia was defined as a total serum bilirubin level that exceeded or was within 1 mg/dL (17.1 μmol/L) of the hour-specific American Academy of Pediatrics threshold for phototherapy. (3) Redrawn from data reported by Keren et al. (7)
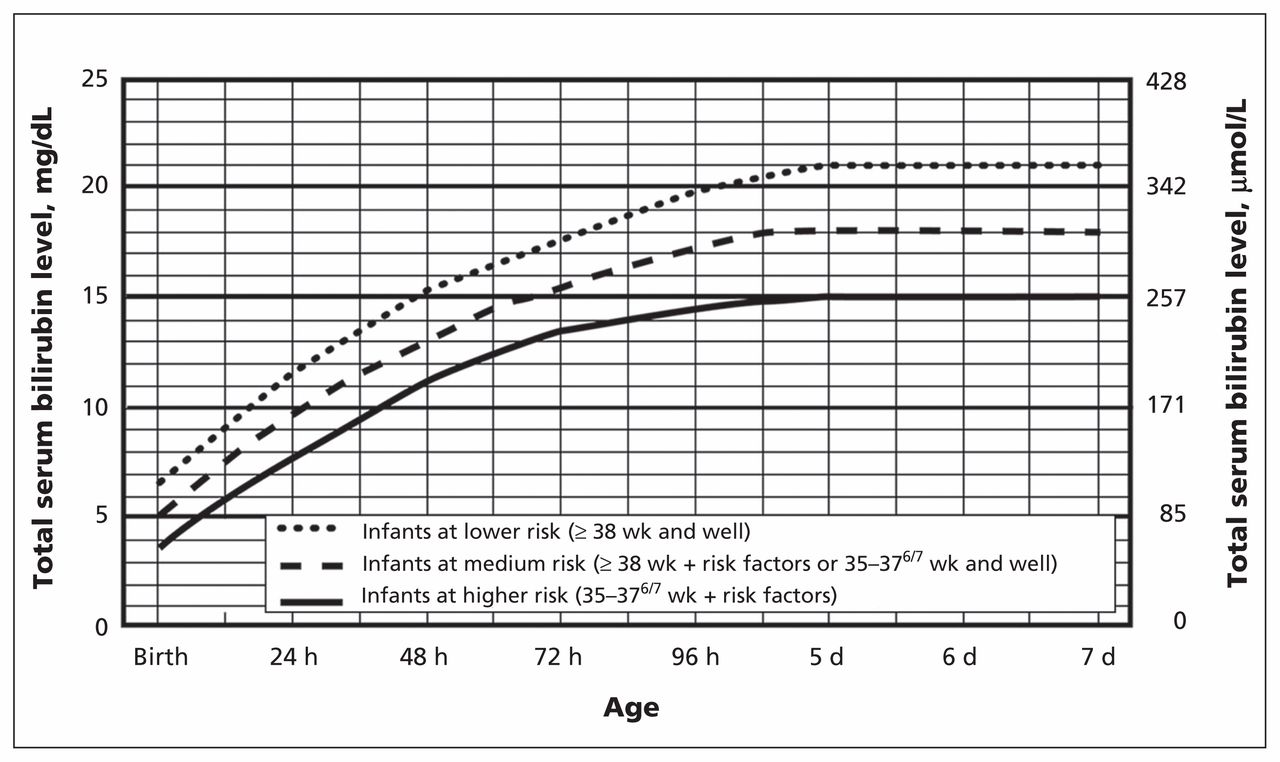
- Figure 4:
Guidelines for phototherapy in inpatient newborns at ≥ 35 weeks’ gestation. Use total serum bilirubin. Do not subtract direct reacting or conjugated bilirubin. The lines for lower, medium and higher risk refer to risk of neurotoxicity (for neurotoxicity risk factors, see Box 4). For well infants at 35 to 376/7 weeks’ gestation, total serum bilirubin levels can be adjusted for intervention around the medium risk line. It is an option to intervene at lower levels for infants closer to 35 weeks’ gestation and at higher levels for infants closer to 376/7 weeks’ gestation. Conventional phototherapy can be provided in hospital or at home at total serum bilirubin levels of 2–3 mg/dL (35–50 μmol/L) below those shown, but home phototherapy should not be used in any infant with risk factors. These guidelines refer to the use of intensive phototherapy, which should be used when the total serum bilirubin level exceeds the line indicated for each category. Infants are designated as higher risk because of the potential negative effects of the conditions listed on albumin binding of bilirubin, (41)– (43) the blood–brain barrier (44) and the susceptibility of the brain cells to damage by bilirubin. (44) Intensive phototherapy implies irradiance in the blue–green spectrum (wavelengths of about 430–490 nm) of at least 30 μW/cm2 per nanometre (measured at the infant’s skin directly below the centre of the phototherapy unit) and delivered to as much of the infant’s surface area as possible. Note that irradiance measured below the centre of the light source is much greater than that measured at the periphery. Measurements should be made with a radiometer specified by the manufacturer of the phototherapy system. If the total serum bilirubin level does not decrease or continues to rise in an infant who is receiving intensive phototherapy, this strongly suggests the presence of hemolysis. Reproduced with permission from Maisels et al., (5) Pediatrics 2009;124:1193–8. Copyright © 2009 American Academy of Pediatrics.




In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
- Article
- Why do newborns become jaundiced?
- What are normal and potentially harmful bilirubin levels?
- How often does kernicterus occur?
- What do the guidelines say?
- Why does kernicterus still occur in the developed world?
- How else might we assess a newborn with jaundice?
- Can we predict which infant will have severe hyperbilirubinemia?
- What is the role of G6PD deficiency in severe hyperbilirubinemia?
- Can we prevent hyperbilirubinemia in breastfed infants?
- How is hyperbilirubinemia treated?
- Conclusion
- Footnotes
- References
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- Regulation of Intestinal UDP-Glucuronosyltransferase 1A1 by the Farnesoid X Receptor Agonist Obeticholic Acid Is Controlled by Constitutive Androstane Receptor through Intestinal Maturation
- Determinants of neonatal jaundice among neonates admitted to five referral hospitals in Amhara region, Northern Ethiopia: an unmatched case-control study
- Glucose-6-Phosphate Dehydrogenase Deficiency and the Benefits of Early Screening
- Humanized UGT1 Mice, Regulation of UGT1A1, and the Role of the Intestinal Tract in Neonatal Hyperbilirubinemia and Breast Milk-Induced Jaundice
- Guidelines on the management of abnormal liver blood tests
- Intestinal NCoR1, a regulator of epithelial cell maturation, controls neonatal hyperbilirubinemia
More in this TOC Section
Similar Articles
Collections

