


Abstract
Background: There is controversy about which children with minor head injury need to undergo computed tomography (CT). We aimed to develop a highly sensitive clinical decision rule for the use of CT in children with minor head injury.
Methods: For this multicentre cohort study, we enrolled consecutive children with blunt head trauma presenting with a score of 13–15 on the Glasgow Coma Scale and loss of consciousness, amnesia, disorientation, persistent vomiting or irritability. For each child, staff in the emergency department completed a standardized assessment form before any CT. The main outcomes were need for neurologic intervention and presence of brain injury as determined by CT. We developed a decision rule by using recursive partitioning to combine variables that were both reliable and strongly associated with the outcome measures and thus to find the best combinations of predictor variables that were highly sensitive for detecting the outcome measures with maximal specificity.
Results: Among the 3866 patients enrolled (mean age 9.2 years), 95 (2.5%) had a score of 13 on the Glasgow Coma Scale, 282 (7.3%) had a score of 14, and 3489 (90.2%) had a score of 15. CT revealed that 159 (4.1%) had a brain injury, and 24 (0.6%) underwent neurologic intervention. We derived a decision rule for CT of the head consisting of four high-risk factors (failure to reach score of 15 on the Glasgow coma scale within two hours, suspicion of open skull fracture, worsening headache and irritability) and three additional medium-risk factors (large, boggy hematoma of the scalp; signs of basal skull fracture; dangerous mechanism of injury). The high-risk factors were 100.0% sensitive (95% CI 86.2%–100.0%) for predicting the need for neurologic intervention and would require that 30.2% of patients undergo CT. The medium-risk factors resulted in 98.1% sensitivity (95% CI 94.6%–99.4%) for the prediction of brain injury by CT and would require that 52.0% of patients undergo CT.
Interpretation: The decision rule developed in this study identifies children at two levels of risk. Once the decision rule has been prospectively validated, it has the potential to standardize and improve the use of CT for children with minor head injury.
Each year more than 650 000 children are seen in hospital emergency departments in North America with “minor head injury,” i.e., history of loss of consciousness, amnesia or disorientation in a patient who is conscious and responsive in the emergency department (Glasgow Coma Scale score 1 13–15). Although most patients with minor head injury can be discharged after a period of observation, a small proportion experience deterioration of their condition and need to undergo neurosurgical intervention for intracranial hematoma. 2–4 The use of computed tomography (CT) in the emergency department is important in the early diagnosis of these intracranial hematomas.
Over the past decade the use of CT for minor head injury has become increasingly common, while its diagnostic yield has remained low. In Canadian pediatric emergency departments the use of CT for minor head injury increased from 15% in 1995 to 53% in 2005. 5,6 Despite this increase, a small but important number of pediatric intracranial hematomas are missed in Canadian emergency departments at the first visit. 3 Few children with minor head injury have a visible brain injury on CT (4%–7%), and only 0.5% have an intracranial lesion requiring urgent neurosurgical intervention. 5,7 The increased use of CT adds substantially to health care costs and exposes a large number of children each year to the potentially harmful effects of ionizing radiation. 8,9 Currently, there are no widely accepted, evidence-based guidelines on the use of CT for children with minor head injury.
A clinical decision rule incorporates three or more variables from the history, physical examination or simple tests10.11 into a tool that helps clinicians to make diagnostic or therapeutic decisions at the bedside. Members of our group have developed decision rules to allow physicians to be more selective in the use of radiography for children with injuries of the ankle 12 and knee, 13 as well as for adults with injuries of the ankle, 14–17 knee, 18–20 head 21,22 and cervical spine. 23,24 The aim of this study was to prospectively derive an accurate and reliable clinical decision rule for the use of CT for children with minor head injury.
Methods
Study setting and population
We conducted a prospective cohort study in 10 Canadian pediatric teaching institutions and enrolled consecutive children (0–16 years of age) if they presented to one of the emergency departments after sustaining an acute minor head injury. Eligibility was based on patients having all of the following: (a) blunt trauma to the head resulting in witnessed loss of consciousness, definite amnesia, witnessed disorientation, persistent vomiting (two or more distinct episodes of vomiting 15 minutes apart) or persistent irritability in the emergency department (for children under two years of age); (b) initial score on the Glasgow Coma Scale in the emergency department of at least 13, as determined by the treating physician; and (c) injury within the past 24 hours. Patients were excluded if they had obvious penetrating skull injury or obvious depressed fracture, acute focal neurologic deficit, chronic generalized developmental delay or head injury secondary to suspected child abuse. Patients who were returning for reassessment of a previously treated head injury and those who were pregnant were also excluded. The research ethics committee of each study hospital approved the study.
Standardized assessment of patients
Staff physicians in the emergency department who were certified in pediatrics, emergency medicine or family medicine or supervised residents (in their second year of training or above) assessed the patients. These physician assessors each underwent a one-hour training session on evaluating patients for 26 standardized clinical findings from the history, general examination and neurologic status. These potential predictor variables had been selected a priori by a team of investigators (M.H.O., T.P.K., A.J., G.J., B.B., L.C.-K., M.P., D.M., C.N.-J., B.T., I.G.S.) on the basis of a review of the existing literature and results of a pilot study. The assessors recorded the findings of the standardized assessment on data collection sheets before any CT. When it was feasible, a second emergency physician independently assessed each patient, to allow determination of interobserver agreement. For patients transferred from a primary care hospital, the study assessments took place after arrival at the study site.
Outcome measures and their assessment
The primary outcome was need for neurologic intervention, and the secondary outcome was brain injury on CT. The need for neurologic intervention was defined as either death within seven days secondary to the head injury or need for any of the following procedures within seven days: craniotomy, elevation of skull fracture, monitoring of intracranial pressure or insertion of an endotracheal tube for the treatment of head injury. Brain injury was defined as any acute intracranial finding revealed on CT that was attributable to acute injury, including closed depressed skull fracture (i.e., depressed past the inner table) and pneumocephalus but excluding nondepressed skull fractures and basilar skull fractures.
After the clinical examination, the treating physician determined whether the patient should undergo CT of the head. Staff radiologists at each site, who were blinded to the content of the data collection form, interpreted the CT scans. If the radiologist raised any uncertainty about whether an acute intracranial injury existed, then another radiologist and a neurosurgeon, both also blinded to the content of the data collection form, reviewed the CT scan. If uncertainty remained, the scan was considered negative.
Because not all patients with minor head injury routinely undergo CT at the study sites, we could not ethically mandate universal CT for all patients included in the study. Patients who did not undergo imaging were classified as having no clinically important brain injury if they met all of the following explicit criteria at 14 days, as determined during a structured interview conducted by telephone: headache absent or mild, complaints of memory or concentration problems absent, seizure or focal motor findings absent and return to usual daily activities (feeding, sleeping, school, play and work). A nurse who was unaware of the patient’s predictor clinical variables assessed these criteria. Patients who did not meet these criteria returned for clinical reassessment and CT. Patients were classified as having brain injury solely on the basis of their CT findings. Patients who did not undergo CT and who could not be reached for follow-up were excluded from the final analysis.
Statistical analysis
We assessed the interobserver agreement for each variable using the kappa statistic and 95% confidence intervals (CIs). We did not calculate kappa values for variables created by cut-point (e.g., amnesia ≥ 30 minutes before injury) or for those collected from the medical record (e.g., age). We used univariable analyses with χ2 tests (or, for age, the t test) to determine the strength of the association of these dichotomous variables with the primary outcome. We used recursive partitioning to combine variables that we found to be both reliable (kappa coefficient > 0.5) and strongly associated with the outcome measures (p < 0.05) to find the best combinations of predictor variables that were highly sensitive for detecting the outcome measure while achieving the maximum possible specificity. Recursive partitioning creates a branching decision tree by dividing the patient population into subgroups with and without the outcome of interest according to the contents of predictor variables in the subgroup. We used KnowledgeSEEKER version 6.0 Software (Angoss Software International) for the recursive partitioning. Our previous experience suggested that recursive partitioning may be more suitable than logistic regression when the objective is to correctly classify one outcome group at the expense of the other (i.e., where high sensitivity is more important than overall accuracy).
We assessed the derived decision rule by comparing the classification of each patient with his or her actual status for the primary outcomes, which allowed us to estimate, with 95% CIs, the sensitivity and specificity of the rule. The bootstrapping method 25 was used to evaluate the classification performance of the decision rule and to assess overfitting of the model.
Results
Characteristics of the patients
Between July 2001 and November 2005, we enrolled 3866 patients, all of whom underwent complete assessment of the primary outcome (Table 1, Table 2). Assessment of the secondary outcome, brain injury on CT, reflected CT findings for 2043 (52.8%) of the patients. The remaining 1823 (47.2%) patients, who were all discharged directly from the emergency department, underwent the structured telephone interview with a registered nurse at 14 days after discharge for determination of the proxy outcome measure. Of all patients included in the study, 24 (0.6%) underwent a neurologic intervention. CT revealed a brain injury in 159 (4.1%) of the patients. The study sample included 277 children under two years of age, and 23 of these had brain injury revealed by CT. An additional 245 eligible patients were not included in the final analysis because they did not undergo CT or the telephone interview at 14 days to determine the proxy outcome measure. The characteristics of these patients were similar to those who underwent CT or the telephone interview to determine the proxy outcome measure. Another 2178 eligible patients were seen at the study sites but were not enrolled by the treating physicians. The characteristics of these non-enrolled patients were similar to those of patients who were enrolled, including mean age (8.4 v. 9.2 years), rate of arrival by ambulance (35.3% v. 38.2%), transfer from another hospital (15.9% v. 17.2%) and mechanism of injury.
Table 1: Characteristics of 3866 children with head injury
Table 2: Management and outcomes for the 3866 patients
Predictor variables
The variables with the highest associations with brain injury were those found on physical examination: suspected open or depressed fracture; signs of basal skull fracture; large, boggy hematoma of the scalp; and low or deteriorating Glasgow Coma Scale score (Table 3, Table 4). The interobserver agreement (n = 333 cases) for some of the primary variables is given in Table 3.
Table 3: Association between variables (from history and physical examination) and presence of brain injury in children with a minor head injury (part 1 of 2)
Table 3: Association between variables (from history and physical examination) and presence of brain injury in children with a minor head injury (part 2 of 2)
Table 4: Association between variables related to mechanism of injury and presence of brain injury in children with a minor head injury
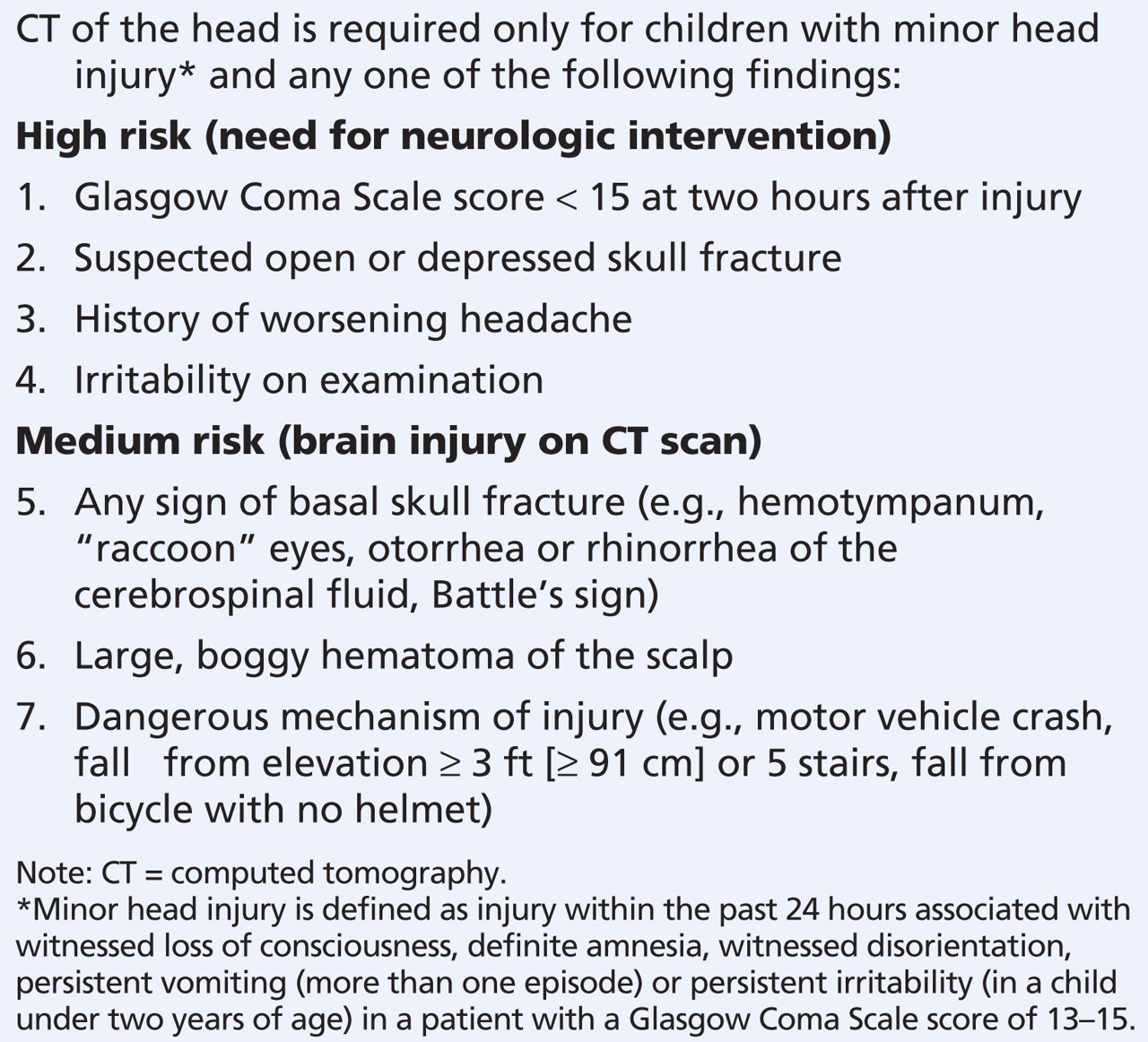
Combining variables using recursive partitioning analyses yielded a rule based on seven simple questions stratified as representing high risk and medium risk. The resulting rule (Box 1) is called the CATCH rule, for Canadian Assessment of Tomography for Childhood Head injury. Having any one of the four high-risk factors predicting the primary outcome, need for neurologic intervention, had a sensitivity of 100.0% (95% CI 86.2%–100.0%) and a specificity of 70.2% (95% CI 68.8%–71.6%) and would require that 30.2% of patients with minor head injury undergo CT (Table 5). The presence of any one of the four high-risk or three medium-risk factors in the rule would identify any CT-visible brain injury with a sensitivity of 98.1% (95% CI 94.6%–99.4%) and a specificity of 50.1% (95% CI 48.5%–51.7%) and would require that 51.9% of patients with minor head injury undergo CT (Table 6). The three cases of brain injury that were not identified by this rule were an occipital skull fracture with a small pneumocephalus, mild brain edema and a small extra-axial hemorrhage (probably epidural) with a small cerebral contusion. None of these patients required treatment, and none had neurologic sequelae.
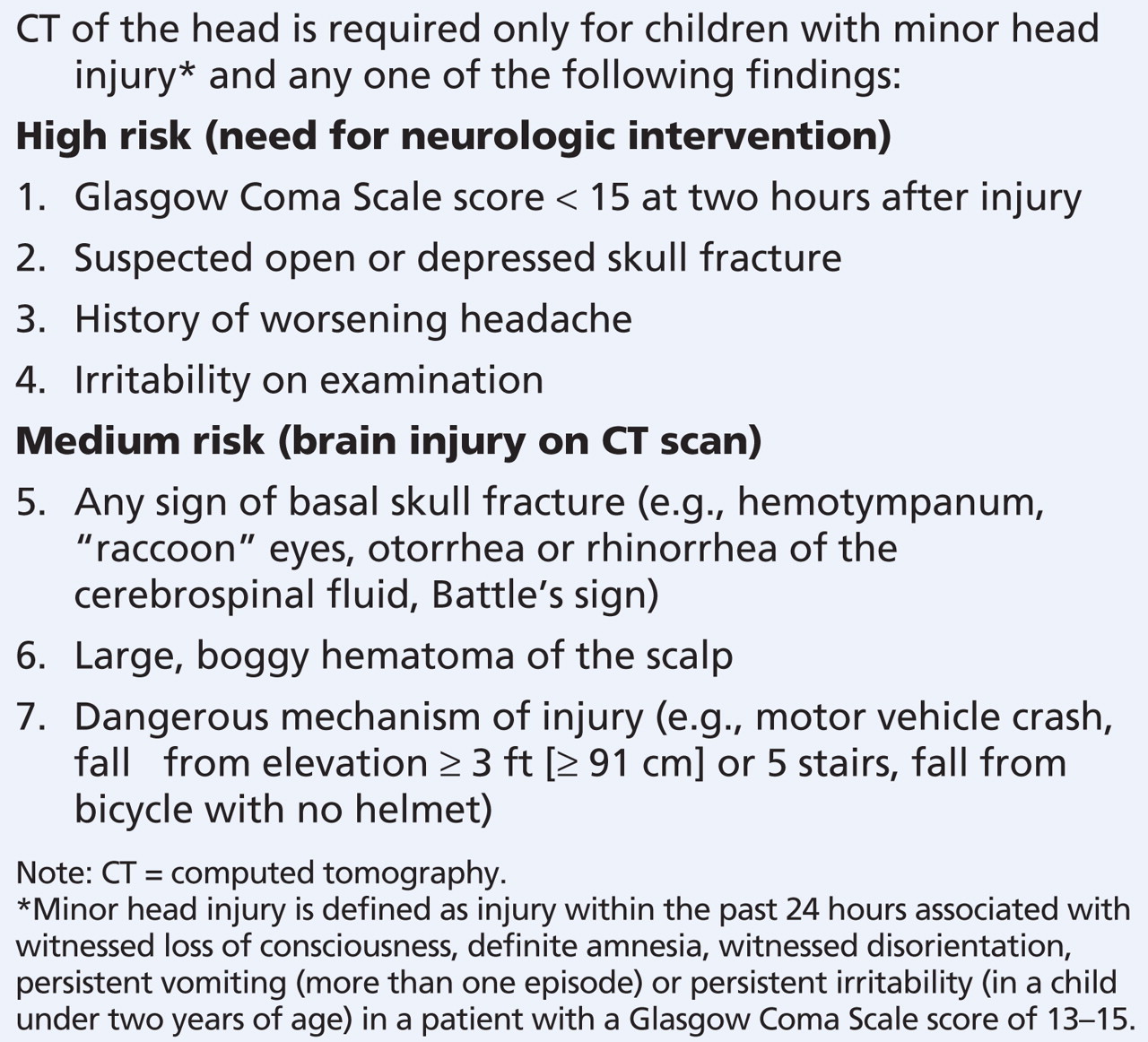
Box 1: Canadian Assessment of Tomography for Childhood Head injury: the CATCH rule
Table 5: Performance of the four high-risk factors in the CATCH rule in relation to need for neurologic intervention in children with a minor head injury
Table 6: Performance of all seven risk factors in the CATCH rule in relation to the presence of brain injury on CT scan in children with a minor head injury
According to the bootstrapping results, the classification performance of the CATCH rules was accurate across 1000 bootstrapped test sets and was consistent with the estimation from the original data set. For the four high-risk factors for neurologic intervention, the sensitivity was 97.9% (95% CI 97.8%–97.9%) and the specificity was 70.2% (95% CI 70.1%–70.3%). For all seven factors determining the risk for brain injury, the sensitivity was 98.1% (95% CI 98.0%–98.2%) and the specificity was 50.0% (95% CI 50.0%–50.1%).
Interpretation
We have developed a clinical decision rule that can be used to identify two levels of risk in children with minor head injury. Patients with any one of four high-risk factors are at significant risk for a need for neurosurgical intervention, whereas patients with any of three additional medium-risk characteristics are at risk of having a brain injury that will be seen on CT. We derived the CATCH rule according to strict methodologic standards and using a large sample of patients. Nevertheless, we intend to prospectively and explicitly validate the rule at multiple sites.
There is considerable disagreement as to the indications for CT in the large number of head trauma cases classified as minor. 26–28 Some support routine CT of all patients with minor head injury who have lost consciousness or have amnesia, 26 wheres others endorse more selective use of CT in cases of minor head injury. 27,28 Without the support of widely accepted, evidence-based guidelines, physicians are likely to follow the conservative approach of ordering CT for most children with minor head injury seen in an emergency department.
A number of studies have been conducted in the past 10 years to identify a set of high-risk findings that would clearly indicate which children with minor head injury should undergo CT. 29–34 Unfortunately, those studies have been highly variable in design, and few could be considered robust according to methodologic standards for the development of clinical decision rules. 11 Interestingly, all of the clinical variables that make up the CATCH rule have been found to be significant predictors of intracranial injury and have been part of clinical decision rules developed in previous studies: Glasgow Coma Scale score less than 15 at two hours, 30–33 suspected open or depressed skull fracture, 30–33 worsening headache, 29,30 persistent irritability, 31 sign of basal skull fracture, 30–33 large, boggy scalp hematoma 31,32 and dangerous mechanism of injury. 32,33
We believe that an accurate decision rule could stabilize or reduce the number of children undergoing CT, thereby minimizing both health care costs and children’s exposure to the potentially harmful effects of ionizing radiation. There is growing concern that early exposure to ionizing radiation may result in a substantial rise in lifetime risk of fatal cancer. Brenner and colleagues 8 estimated that the lifetime cancer mortality risk attributable to the ionizing radiation to which a one-year-old child would be exposed through a single CT scan of the head was about 1 in 1500; they estimated the corresponding mortality risk for 10-year-olds as about 1 in 5000. In addition, Hall and others 9 recently reported that low doses of ionizing radiation to the brain in infancy may influence cognitive abilities in adulthood. These risks may be small for a given individual, but when applied to a large population they may create a substantial public health risk.
Limitations
Our study had potential limitations. For ethical reasons, not all enrolled children with minor head injury underwent CT. Nonetheless, we are confident that the children who did not undergo CT received a full assessment for the primary outcome measure, the need for neurologic intervention. All of the study patients who were not examined by CT did undergo a structured and validated telephone interview at 14 days for determination of the proxy outcome measure. Any patient who could not be completely and adequately followed was excluded from the study analyses. Although not all children with minor head injury seen at the study sites during the study period were enrolled in the study, this situation is not out of the ordinary for a clinical study, and we could not determine any systematic difference between the patients who were enrolled and those who were not enrolled. We enrolled relatively few children under two years of age (n = 277), and we identified only 23 cases of brain injury in this group. Although the CATCH rule correctly identified all these cases of brain injury, further prospective study of this subgroup is required, as children under two years of age may have more subtle presentations of head injury than older children. 28,35
Some may question the significance of relatively small lesions found on the CT scans. In our study we defined as significant any intracranial bleeding or contusion seen on CT, no matter how small, as well as isolated pneumocephalus seen on CT. We consulted several Canadian academic pediatric neurosurgeons, all of whom felt that any abnormality caused by acute trauma is important in children. However, we recognize that there is no consensus among health care professionals on this issue. Additional studies are needed to evaluate the clinical significance of these very small lesions and to evaluate whether finding them justifies the risk associated with exposing the child to radiation. Finally, before it can be used in clinical practice, this derived rule must be prospectively validated to determine its accuracy, its acceptability to clinicians and its impact on care in a new patient population. 36,37
Conclusion
The CATCH rule is a sensitive, prospectively derived clinical decision rule that has the potential to both standardize the need for CT and reduce the number of CT scans performed for children with minor head injury. Further studies are required to prospectively validate this rule in other pediatric cohorts.
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: None declared. George Wells is a biostatistical consultant for CMAJ and was not involved in the editorial decision-making process for this article.
Contributors: All of the authors contributed to the conceptual design of the study. Rhonda Correll, Anna Jarvis, Gary Joubert, Benoit Bailey, Laurel Chauvin-Kimoff, Martin Pusic, Don McConnell, Cheri Nijssen-Jordan, Norm Silver and Brett Taylor contributed to the acquisition of data. Martin Osmond, Terry Klassen, George Wells and Ian Stiell contributed to the analysis and interpretation of the data and to drafting the manuscript. All of the authors critically reviewed the article for important intellectual content and approved the final version submitted for publication.
Funding: This study was funded by peer-reviewed grants from the Canadian Institutes of Health Research (CIHR funding reference number MOP-43911), the Emergency Health Services Branch of the Ontario Ministry of Health and Long-Term Care and the Alberta Children’s Hospital Foundation.
Acknowledgements: The authors thank the other members of the Pediatric Emergency Research Canada (PERC) Head Injury Study Group, Dr. Martin Reed (University of Manitoba), Dr. Keith Aronyk (University of Alberta), Dr. Michael Vassilyadi (University of Ottawa) and Dr. Mark Hamilton (University of Calgary), for their assistance with study design and interpretation of data. We thank the following for their much-appreciated assistance as the study coordinators at each site: Jennifer Spruyt, Eleanor Fitzpatrick, Rita Arsenault, Bev Irwin, Rose Jacobson, Sue Heathcote, Lanna Bryksa, Nathalie Franc, Geri St Jean and Diane Laforte. The authors thank My-Linh Tran and Sheryl Domingo for managing the data. The authors also thank all of the physicians, nurses and clerks at the study sites who voluntarily assisted in identifying cases and collecting data.
REFERENCES
In this issue
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Validation of the Scandinavian guidelines for minor and moderate head trauma in children: protocol for a pragmatic, prospective, observational, multicentre cohort study
- Which elements of hospital-based clinical decision support tools for the assessment and management of children with head injury can be adapted for use by paramedics in prehospital care? A systematic mapping review and narrative synthesis
- Limiter les tomodensitometries inutiles pour une commotion cerebrale pediatrique
- Curb unnecessary computed tomography scans for pediatric concussions
- Cost-effectiveness of patient observation on cranial CT use with minor head trauma
- Radiographies du crane apres un traumatisme cranien mineur chez les enfants de moins de 2 ans
- Skull x-ray scans after minor head injury in children younger than 2 years of age
- Postauricular swelling secondary to salmonella extradural abscess in a toddler: a near miss condition
- Reducing unnecessary CT scan of the head for minor paediatric head injuries at the emergency department
- Evidence base for point-of-care ultrasound (POCUS) for diagnosis of skull fractures in children: a systematic review and meta-analysis
- Head home: a prospective cohort study of a nurse-led paediatric head injury clinical decision tool at a district general hospital
- Kids Outcomes And Long-term Abilities (KOALA): protocol for a prospective, longitudinal cohort study of mild traumatic brain injury in children 6 months to 6 years of age
- Codesigning discharge communication interventions with healthcare providers, youth and parents for emergency practice settings: EDUCATE study protocol
- Association of clinically important traumatic brain injury and Glasgow Coma Scale scores in children with head injury
- Use of CT in children with minor head injuries with isolated vomiting
- Traumatic brain injury in young children with isolated scalp haematoma
- Multicentre, randomised clinical trial of paediatric concussion assessment of rest and exertion (PedCARE): a study to determine when to resume physical activities following concussion in children
- Accuracy of NEXUS II head injury decision rule in children: a prospective PREDICT cohort study
- Overall Approach to Trauma in the Emergency Department
- Think A-Head Campaign of Image Gently: Shared Decision-Making in Pediatric Head Trauma
- Validation and refinement of a clinical decision rule for the use of computed tomography in children with minor head injury in the emergency department
- Neuroimaging Wisely
- Selecting children for head CT following head injury
- Diagnostic performance of S100B protein serum measurement in detecting intracranial injury in children with mild head trauma
- Trends in admission and death rates due to paediatric head injury in England, 2000-2011
- Derivation and validation of a clinical decision rule to identify young children with skull fracture following isolated head trauma
- Managing isolated head trauma in young children
- Head injury from falls in children younger than 6 years of age
- Physician practice and PECARN rule outperform CATCH and CHALICE rules based on the detection of traumatic brain injury as defined by PECARN
- Guidelines for mild head injuries in children
- Vomiting Alone May Not Indicate Serious Pediatric Brain Injury
- Office management of mild head injury in children and adolescents
- Prise en charge en cabinet des lesions cerebrales traumatiques legeres chez les enfants et les adolescents
- Diagnosis and acute management of patients with concussion at children's hospitals
- Applicability of the CATCH, CHALICE and PECARN paediatric head injury clinical decision rules: pilot data from a single Australian centre
- Predicting and preventing postconcussive problems in paediatrics (5P) study: protocol for a prospective multicentre clinical prediction rule derivation study in children with concussion
- Cancer risk in 680 000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians
- Safety and efficacy of symptom-driven CT decision rule in fully conscious paediatric patients with symptoms after mild closed head trauma
- Comparing CATCH, CHALICE and PECARN clinical decision rules for paediatric head injuries
- Pediatric Head Injury
- Vomiting--is this a good indication for CT head scans in patients with minor head injury?
- Minor Head Injury: The CATCH Clinical Decision Rule
- Children with brain injuries
More in this TOC Section
Similar Articles

