


What's your call?
MRIs of the spine of a 54-year-old man with a history of glioblastoma multiforme, who presented with new urinary frequency and urgency, thoracic-to-lumbar back pain and inability to walk.
Intradural extramedullary spinal metastases that arise from intracranial lesions are called drop metastases. This rare complication occurs in about 1% of patients who have glioblastoma multiforme (GBM), the most common form of malignant primary brain tumour (Fig. 1). The mechanism of spread is thought to be via cerebrospinal fluid when the tumour reaches and exfoliates cells into the subarachnoid space. Interventions such as surgical manipulation may enhance the likelihood of drop metastases, although it has also been reported in people who have never had surgery.

Fig. 1: MRI of the patient's brain, T1-weighted, with gadolinium.
Perhaps because of gravitational effects, these lesions typically occur in the dorsal lower-thoracic to lumbar spine (Fig. 2). Nerve roots, cauda equina, nerve root sleeves and the fundus of the thecal sac are also common sites of spread (Surg Neurol 1991;35:377–80). Most patients will complain of back pain with neurologic symptoms and signs.
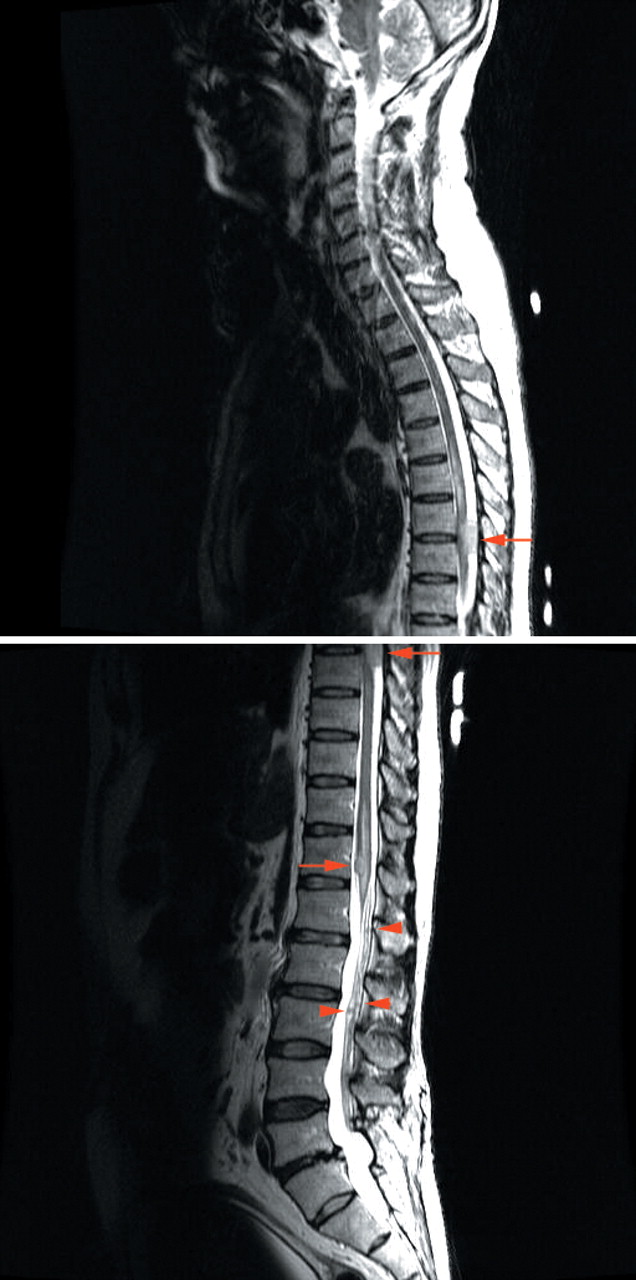
Fig. 2: T2-weighted spinal MRIs. The 2 largest lesions are visible at the mid-T7–T8 and the T12 levels. Several smaller nodules can also be seen within the cauda equina.
Because the lesions may be missed on x-ray films and sometimes on CT scans, the investigative method of choice is spinal MRI with contrast.
Depending on the location, size and number of lesions, the management of drop metastases may include neurosurgery, radiation and steroid therapy. However, the prognosis of such patients is poor.
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

