


A 44-year-old previously healthy woman presented to her primary care physician with a 4-week history of dry cough. She had a 27-pack-year smoking history. There was no history of shortness of breath, chest pain, hemoptysis, fever, night sweats or weight loss. She had travelled to Mexico, South Carolina and the Dominican Republic in the 2 years before the current illness. Physical examination and routine laboratory investigations, including complete and differential blood counts, were normal. A chest radiograph revealed a nodular opacity within the anterior aspect of the right upper lobe of the lung (Fig. 1, arrow).

Figure 1. Photo: Images courtesy of the Departments of Pathology and Molecular Medicine (HRLMP) and of Diagnostic Imaging, St. Joseph's Healthcare, McMaster University
The patient was admitted to a tertiary care hospital to undergo a right upper-lobe wedge resection. Examination of the gross specimen through serial sections revealed a well-circumscribed coin lesion that measured 1.4 cm in diameter. Histopathologic examination revealed pulmonary infarction with central coagulative necrosis surrounded by a dense, fibrous capsule of mature granulation tissue. A focus of foreign material was noted at the centre of the lesion. The material was located entirely within a small pulmonary artery. A parasite resembling the immature form of Dirofilaria immitis was identified on the histopathologic slides (Fig. 2). The diagnosis of pulmonary dirofilariasis was confirmed by a parasitologist at the US Centers for Disease Control and Prevention, Atlanta.
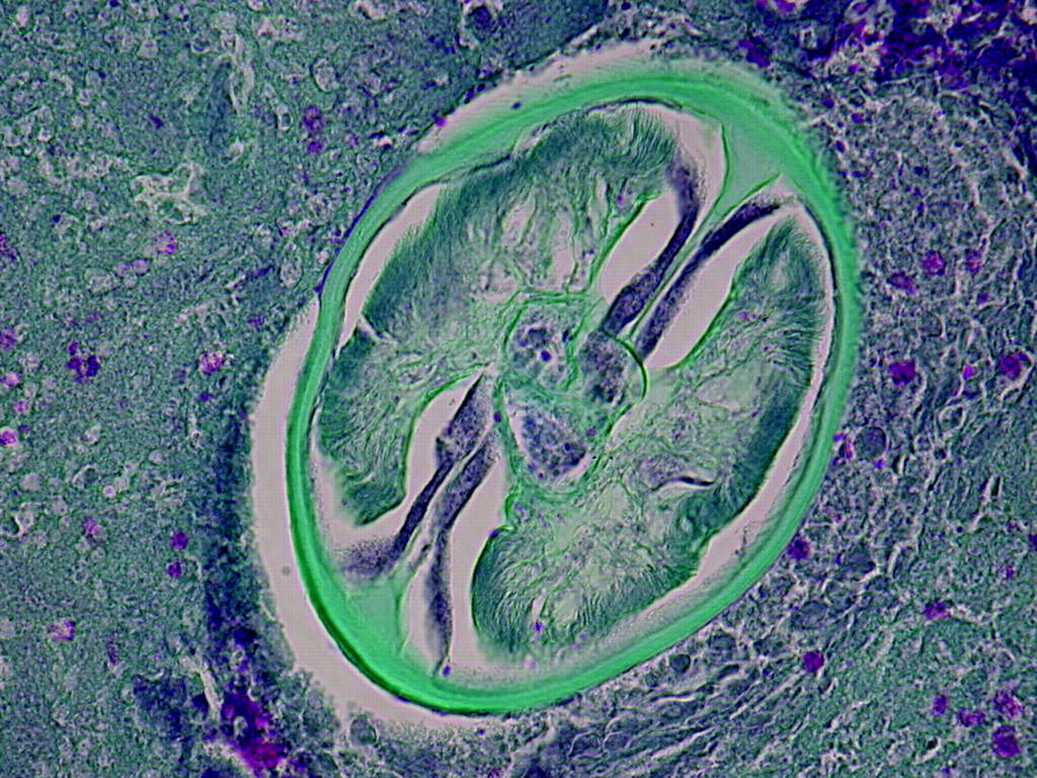
Figure 2. Photo: Images courtesy of the Departments of Pathology and Molecular Medicine (HRLMP) and of Diagnostic Imaging, St. Joseph's Healthcare, McMaster University
The results of 3 different tests of the patient's serum to detect circulating D. immitis antigen (DiroCHEK and Witness Canine Heartworm Antigen Test Kits, Synbiotics Corporation, San Diego, and SNAP Heartworm Antigen Test, Idexx Laboratories, Westbrook, Me.) were negative. The patient recovered completely without treatment.
The heartworm D. immitis is a ubiquitous parasite of dogs found in many temperate parts of the world.1 It is transmitted from an infected dog through the aspiration of circulating microfilariae — the prelarval stage of the parasite — by many species of mosquitoes. The microfilariae mature in the mosquito to third-stage larvae, which may then be transmitted by bite to other dogs, domestic cats, wild canines and humans. The larvae develop in subcutaneous tissues and migrate to the right side of the heart and pulmonary arteries, where they mature into adult parasites. In dogs, the adult worms produce microfilariae that circulate in the blood.2 In humans, D. immitis is generally unable to complete maturation, dies and forms an embolus in the lungs. Thus, human disease is not associated with microfilaremia or other clinical consequences. The negative results of the dirofilarial antigen tests in our case are consistent with the presence of only immature parasites. However, a low burden of mature parasites may produce similar results.
Human pulmonary dirofilariasis characteristically manifests as a solitary pulmonary nodule, which is easily confused with cancer. About 120 cases were reported in the United States between 1941 and 2000, and 60% of patients with pulmonary dirofilariasis are asymptomatic.3 Human cases in Canada are uncommon and are usually the result of travel to an endemic area. Symptomatic patients may experience pleuritic chest pain, cough or hemoptysis.4 Peripheral eosinophilia occurs in less than 15% of cases. Chest radiographs usually show a noncalcified, well-circumscribed peripheral coin lesion.5
The focal pulmonary infarct secondary to D. immitis infection differs in shape from the classic thromboembolic infarct. The latter is pyramidal, and the former is spherical, generally attributed to the centrifugal diffusion of parasite antigen from the degenerating worm.6 The histologic features described in our case are typical.5,7
Most symptomatic cases of human pulmonary dirofilariasis are investigated by means of lung resection to rule out bronchogenic carcinoma.2 Although the natural history of pulmonary dirofilarial granuloma is not well known, it is believed that lesions ultimately calcify.4 No specific therapy for pulmonary dirofilariasis is required.
Danny D. Lagrotteria Department of Medicine McMaster University Hamilton, Ont. Mark A. Crowther Christine H. Lee Department of Molecular Medicine St. Joseph's Healthcare Hamilton, Ont. Andrew Peregrine Ontario Veterinary College Guelph, Ont.
In this issue
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

