


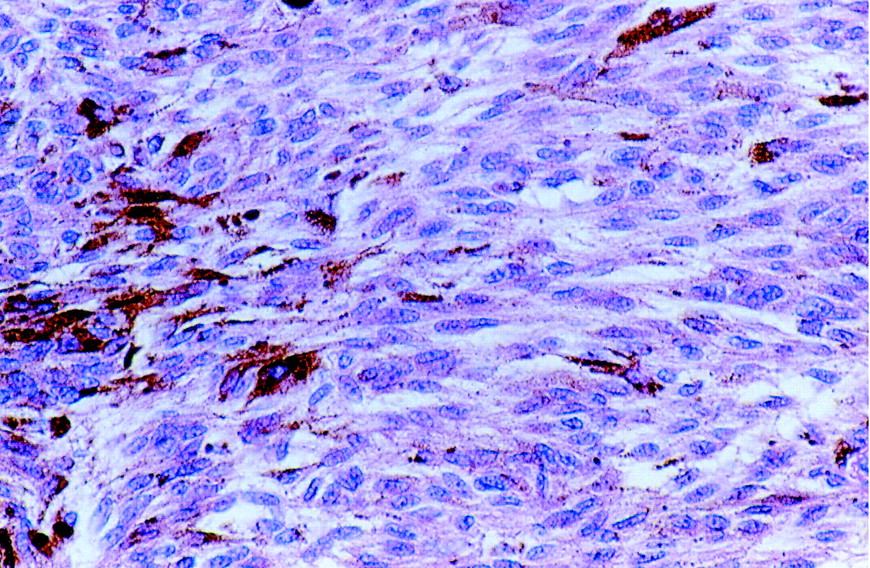
A previously well 71-year-old woman with no prior history of malignant skin cancer was referred to our dermatology clinic because of a large, pedunculated, vegetating lesion in her intergluteal region. The lesion had been present for about 30 years and had been “flat.” However, in recent years it had grown slowly and steadily and, in the few months before presentation, had rapidly increased in size. It was not painful, but there was a slight serosanguineous secretion. The lesion was dome-shaped, with a polypoid appearance, was 4 х 3.5 cm in diameter and was raised 2 cm (Fig. 1). It had a macular smooth surface and greyish-blue colour and was of a tenso-elastic consistency. There were areas of ulceration (up to 1 cm in diameter) and a hemorrhagic fundus with raised margins. The woman had no lymphadenopathy. Because of her age, the lesion's erosions and its recent evolution, a polypoid melanoma was considered, and the lesion was excised deeply with 2-cm margins. Histopathological examination showed fascicles of spindle and epithelioid cells intermingled with dendritic melanocytes and numerous melanophages consistent with a diagnosis of cellular blue nevus (Fig. 2).

Figure 2. Photo: Images courtesy of the Department of Dermatology, University of Florence

Figure 1. Photo: Images courtesy of the Department of Dermatology, University of Florence
The postoperative course was uncomplicated, and the patient was well and disease free at 1 year follow-up.
Blue nevi usually occur on the skin, although they have occasionally been observed on mucous membranes. There are essentially 2 types: common blue nevi and cellular blue nevi (CBN). The former are usually solitary (but can be multiple in number), asymptomatic, blue or black in colour, dome-shaped and less than 1 cm in diameter and, in 50% of cases, occur on or near the dorsa of the hands and feet.
CBN, the rarer variant, are usually solitary, slow growing, 1–3 cm in diameter and deep blue-black or grey in colour and have symmetrical, well-defined edges and a smooth surface. CBN are melanocytic nevi that often resemble malignant melanoma both clinically and histopathologically. They are usually situated in the superficial and middle layers of the dermis but occasionally involve the deep dermis and subcutaneous fat.1,2 Rarely are they ulcerated, but there may be areas of cysto-hemorrhagic degeneration. CBN are most often found in the sacrococcygeal and buttock regions but may also be located on the head or on the dorsa of the hands and feet. They usually are first identified in people under the age of 40, with no difference in incidence between men and women.
The differential diagnosis of CBN includes 2 clinical-histopathological forms. The first, “atypical” CBN, are not considered malignant. They have some atypical cells, often with prominent nucleoli but infrequent mitotic figures. “Malignant” CBN involve more aggressive lesions with infiltrating borders, sheet-like growth, some necrosis, frequent mitoses, nuclear pleomorphism and hyperchromasia.2,3,4
For these reasons, lesions suspected of being CBN must be surgically excised deeply into the subcutaneous tissue and with wide skin margins (at least 0.5 cm) to ensure complete removal and proper pathological distinction of simple CBN from the more aggressive subtypes and malignant melanoma.
Vincenzo de Giorgi Department of Dermatology Daniela Massi Department of Pathology and Human Oncology Serena Sestini Barbara Alfaioli Paolo Carli Department of Dermatology University of Florence Florence, Italy
In this issue
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

