


A male infant was born at term to a woman in her 20s after an uneventful pregnancy and uncomplicated vaginal delivery. He weighed 3500 g and had normal Apgar scores. A large, intact thoracolumbar myelomeningocele was present. There was no family history of neural tube defects, and no specific antenatal testing for these defects had been carried out. The myelomeningocele was associated with a complete sensorimotor paraplegia, absent anal tone, a neurogenic bladder and equinus deformities of the feet. A CT scan of the head performed within days after birth showed hydrocephalus associated with Chiari's malformation type II. At 5 days the myelomeningocele was repaired, and several days later a ventriculoperitoneal shunt was inserted.
At age 4 months the infant presented with a shunt infection, which was treated by removal of the shunt apparatus, external ventricular drainage and appropriate antibiotic therapy. At this time a CT scan showed no evidence of subdural hematomas. When the cerebrospinal fluid became sterile, a new ventriculoperitoneal shunt was inserted. At 10 months, the boy was asymptomatic with a functioning shunt. A CT scan, carried out to assess the ventricular size and the position of the shunt catheter, revealed bilateral subdural hematomas with dense calcification, particularly prominent within the inner membrane (Fig. 1). Because the boy was asymptomatic, surgery was not contemplated. He was followed regularly as an outpatient and continued to be well with normal development, but he was lost to follow-up at age 2 years.
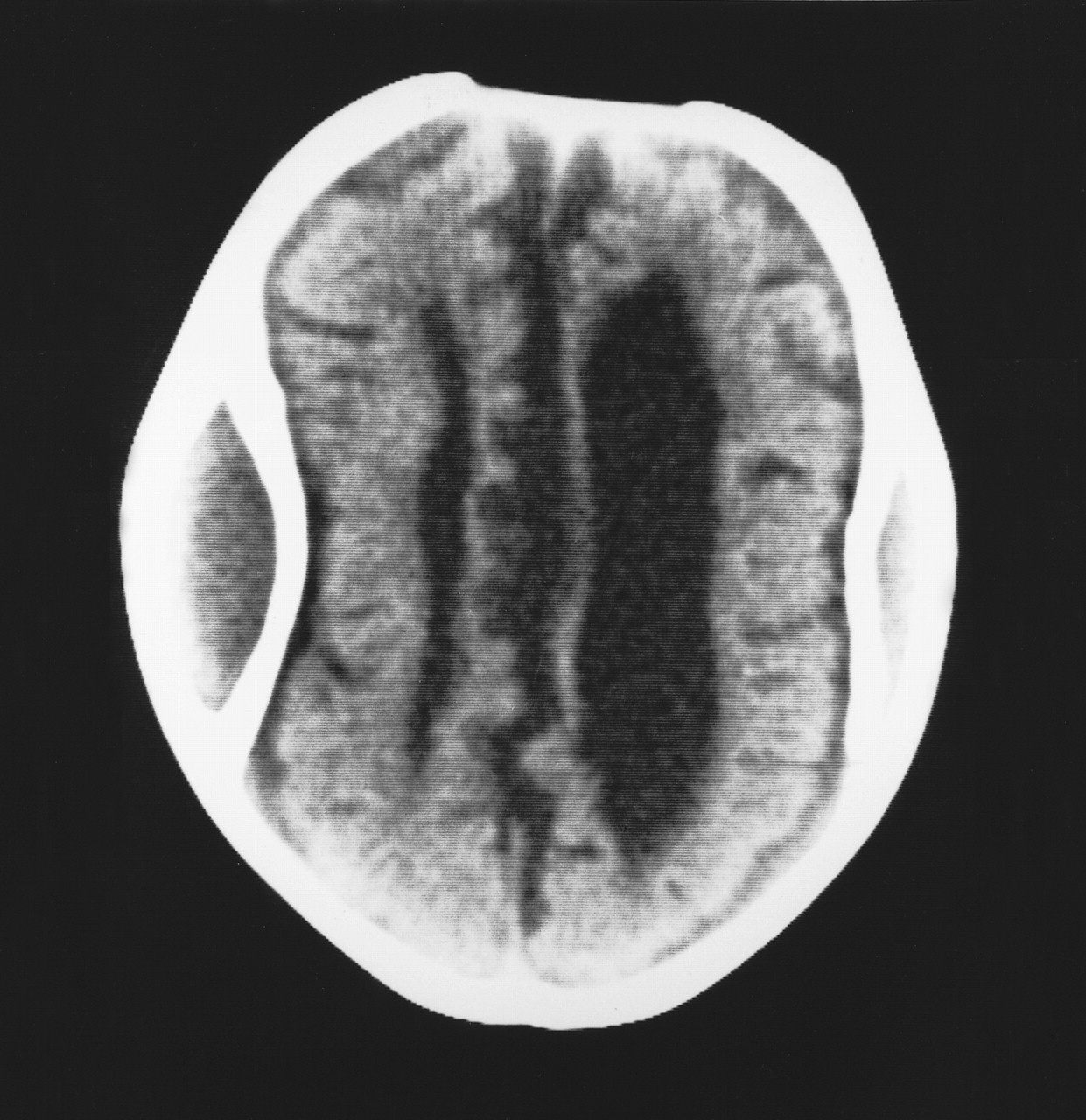
Figure 1. Photo: Image courtesy of Audio Visual Services, King Fahad National Guard Hospital
Dense calcification and even ossification of a chronic subdural hematoma is rare but has been well documented.1 When extensive, it has been likened to a shell or carapace, encasing the brain, thus the term “armoured brain.”2 The frequency with which radiologically demonstrable calcification occurs within the membranes of a chronic subdural hematoma has been reported to range from 0.3% to 2.7%.3 However, Harwood-Nash4 recorded a 10% incidence among children with chronic subdural hematomas studied by plain radiographs. Although usually seen in subdural hematomas resulting from trauma, it has also been reported in post-meningitic subdural effusions as well as subdural hematomas associated with ventricular shunting.5 The latter condition may occur because of a partial collapse of the brain when the intraventricular pressure is reduced by the shunt; this collapse results in widening of the subdural space and stretching of the bridging veins, which thereby increases the risk of hemorrhage.4 Although calcification of subdural hematomas seems more common in children, it has been reported in all age groups.1 The interval between the occurrence of the hematoma and the development of the calcification varies from 6 months to many years.1 , 5 Our patient had a normal CT scan at age 4 months; however, bilateral calcification was evident 6 months later.
The mechanism underlying the calcification remains unclear. Microscopic calcium deposits can often be found within the membranes of a chronic subdural hematoma, in its final stages of development.1 In certain cases, this mineralization may progress to more extensive calcification and even ossification.1 , 3 Etiological theories include poor circulation and delayed absorption of the hematoma fluid within the subdural space, which leads to stagnation and eventually calcification.3 In addition, an underlying metabolic abnormality such as an inherent tendency to calcification has been postulated.1 , 5 The clinical presentation varies, from patients who are asymptomatic to those with symptoms and signs of raised intracranial pressure as well as seizures and mental retardation.1 , 3 , 5
Surgical removal of the calcification is difficult.3 It should not be performed routinely; instead, it should be reserved for patients who have progressive neurological abnormalities or evidence of increased intracranial pressure.
Mohammed Al Wohaibi Neville Russell Ahmad Al Ferayan Division of Neurosurgery King Fahad National Guard Hospital Riyadh, Saudi Arabia
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

