


A previously well 71-year-old woman with a history of cigarette smoking presented to the emergency department with a 6-hour history of dyspnea and pleuritic right-sided chest pain. Her oxygen saturation was 93% on room air, and an electrocardiogram was normal aside from a sinus tachycardia (heart rate 108 beats/min). Her initial chest radiograph appeared normal, and a subsequent ventilation-perfusion scan was of intermediate probability for pulmonary embolism. Heparin was administered, and CT pulmonary angiography was performed later that day using a multidetector helical CT scanner and intravenous contrast medium. The digital scout film (Fig. 1) showed a new peripheral wedge-shaped opacity associated with an infarct in the right lung (Hampton's hump [arrow]). A 2-dimensional reconstruction of the axial CT data was obtained using the maximum intensity projection (MIP) technique (whereby a volume of data is projected in 2 dimensions, showing only the most attenuating, or brightest, objects) in the oblique coronal orientation (Fig. 2). It demonstrated a dark filling defect of a pulmonary embolus extending into the lateral segmental arterial branch of the right middle lobe (arrow). The patient's symptoms gradually resolved with continued anticoagulation, and she was discharged home.
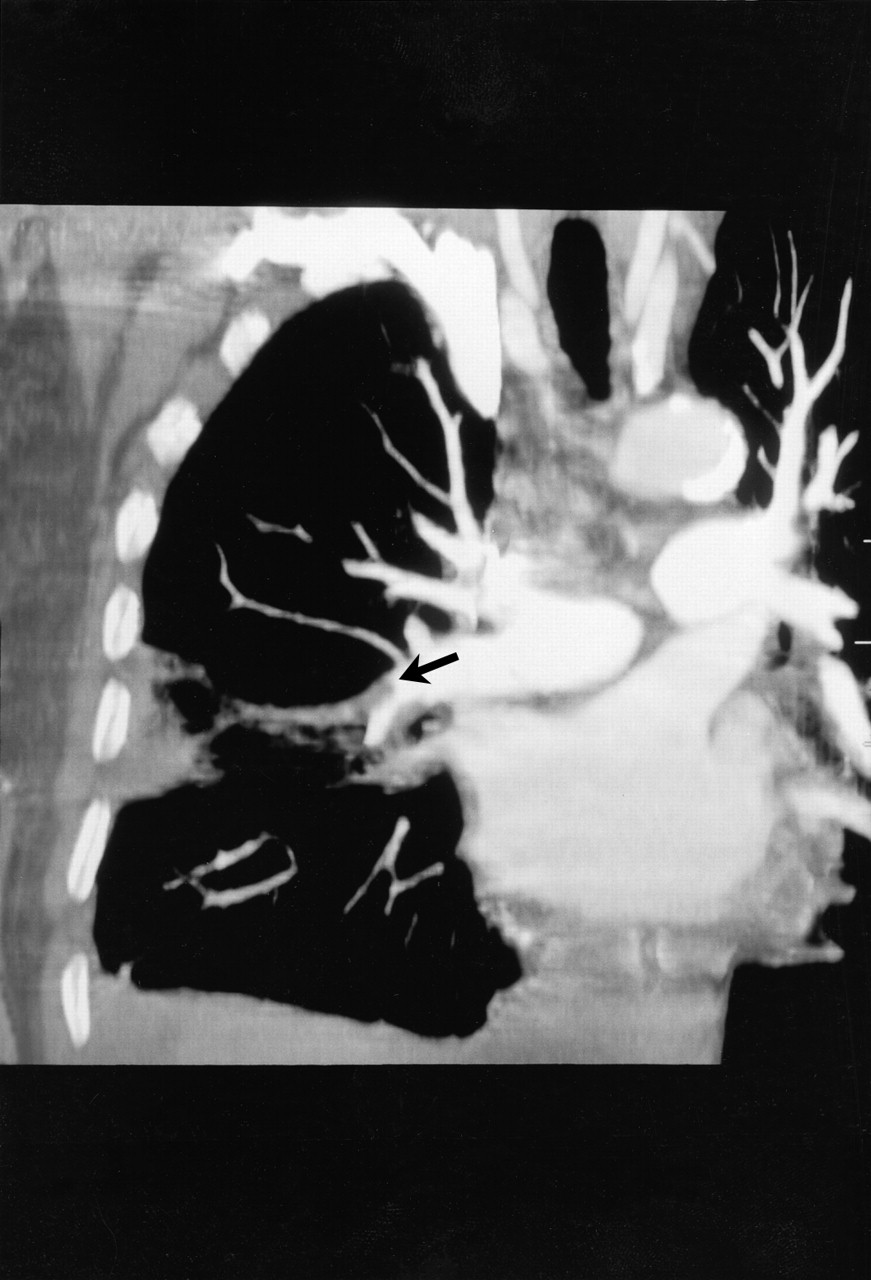
Figure 2. Photo: Courtesy: Iain D.C. Kirkpatrick

Figure 1. Photo: Images courtesy Iain D.C. Kirkpatrick and Michael P. Meyers
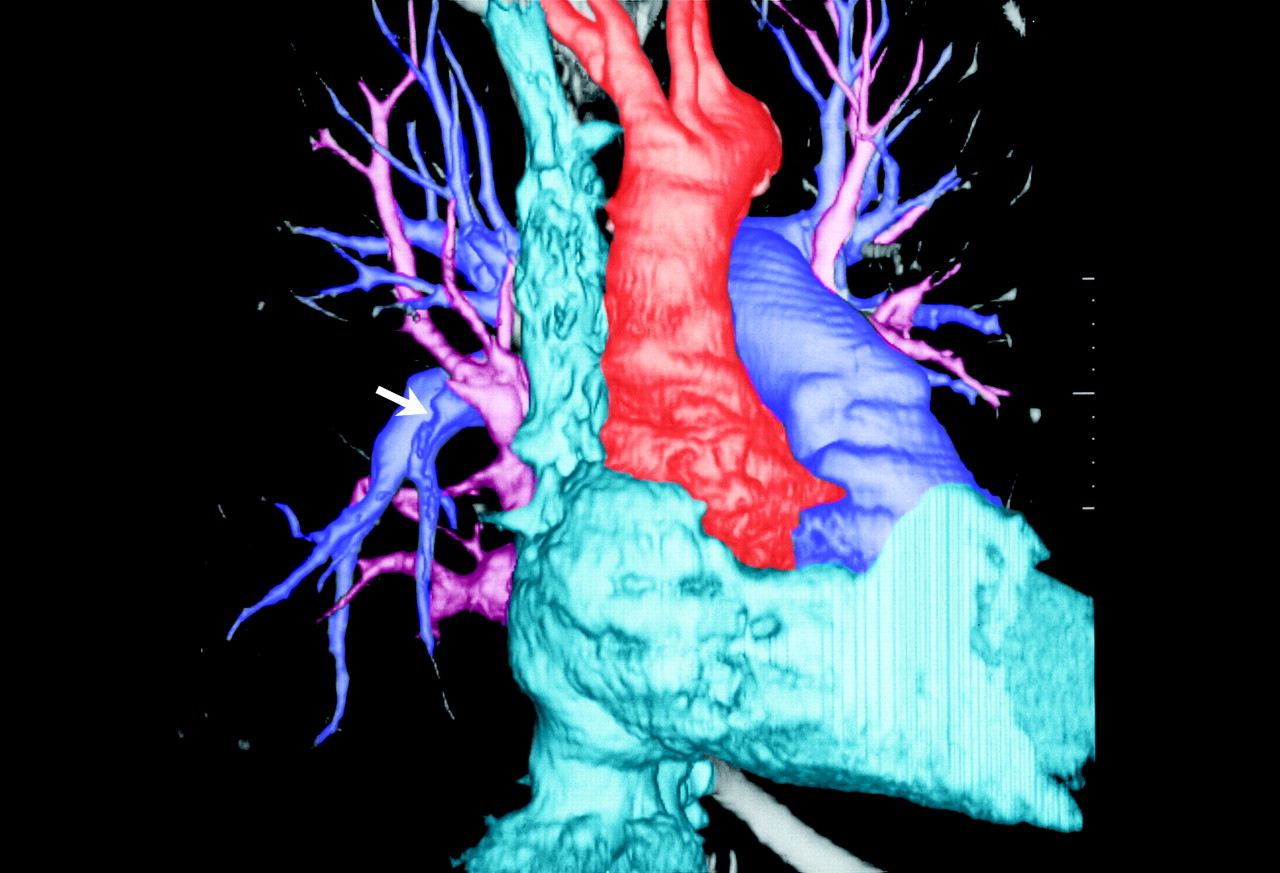
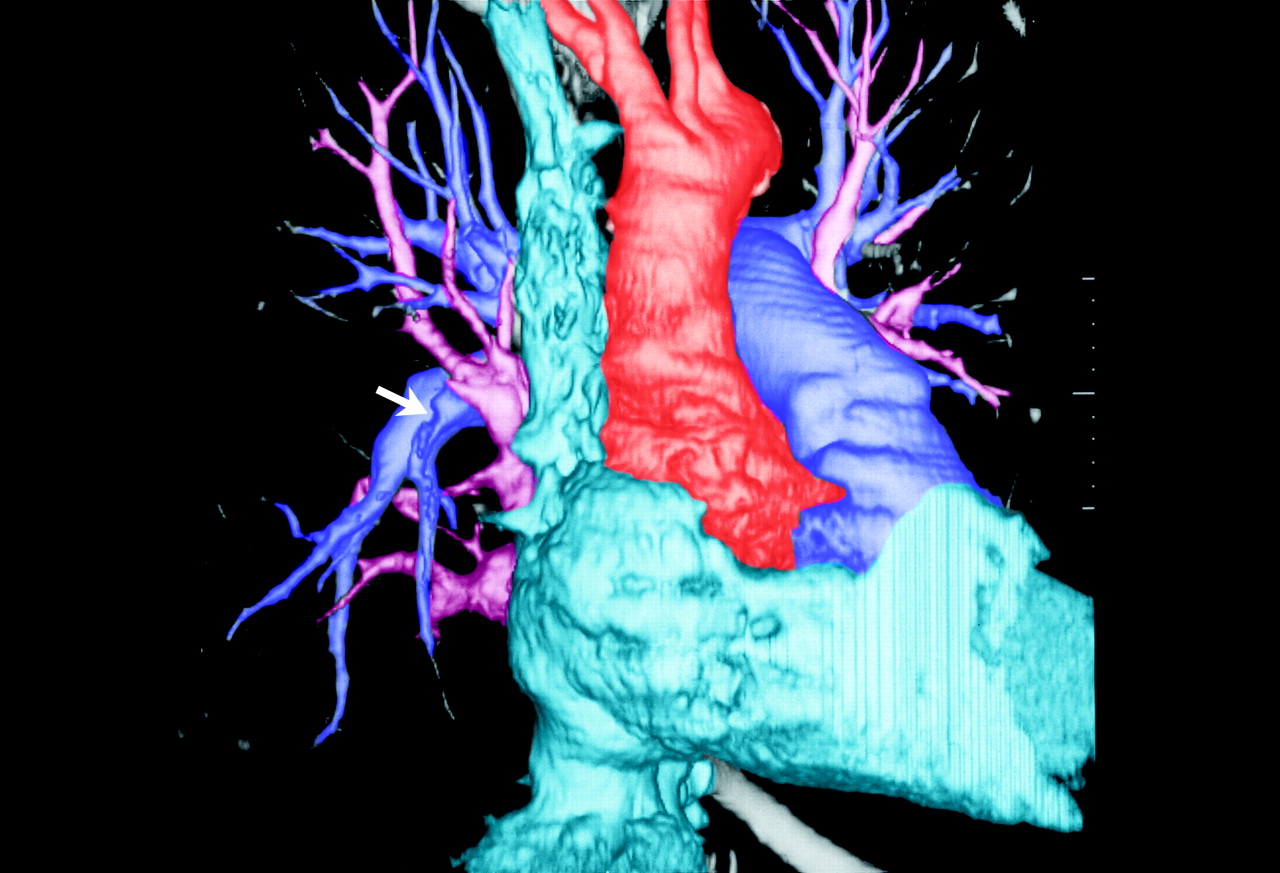
A 3-dimensional volume-rendered image was constructed from the CT data (Fig. 3), allowing only the contrast-filled heart and vasculature to be viewed. (In this colourized version of the image, the superior vena cava and right heart appear in blue, the pulmonary arteries are purple, the pulmonary veins are pink, and the aorta is red). The embolus is represented indirectly by a small meniscus at the origin of the affected pulmonary artery (arrow), ablating the arterial branch, much as it would appear on a conventional pulmonary angiogram. The embolus itself is not seen because of its low x-ray attenuation relative to the iodinated contrast medium.
{kind=link}
{kind=link}
{kind=link}
Figure 3. Photo: Courtesy: Iain D.C. Kirkpatrick
This case demonstrates a range of classic, contemporary and possible future imaging techniques of pulmonary embolism, each with its own strengths and weaknesses. Although the Hampton's hump is one of the classic radiographic findings of pulmonary embolism, conventional chest radiography is rarely helpful in making the diagnosis except to exclude other causes of a patient's symptoms. Catheter pulmonary angiography remains the gold standard for diagnosis;1 however, access to this procedure is often limited, it is invasive, and interobserver agreement is suboptimal for subsegmental vessels.2,3 Ventilation–perfusion scintigraphy is a safe, noninvasive test for classifying patients as being at low, intermediate or high probability of having a pulmonary embolism. Although a low-probability scan virtually rules out pulmonary embolism, further imaging is required if a low- or intermediate-probability scan is obtained but there is a strong clinical suspicion of pulmonary embolism.4 In addition, underlying lung disease often decreases the likelihood of a diagnostic finding with this technique.
Current helical CT technology uses multiple x-ray detectors to allow rapid imaging of smaller vessels (e.g., subsegmental arteries) and reduce motion artifact. Two-row multidetector helical CT units have a sensitivity of 90% and a specificity of 94% with improved interobserver agreement relative to pulmonary angiography;5,6 4- and 8-row units, now in widespread use, should only improve on this performance.
The high-resolution images produced with helical CT allow computerized reformatting of the data in multiple planes beyond the conventional transverse orientation, thus improving the identification of vessels, artifacts and extent of the embolism.7,8,9 The MIP reconstruction technique demonstrated in Fig. 2 lends itself well to CT angiography, since intravenous contrast medium within patent vessels generally makes them quite visible. However, any tissue that is in front of or behind the most dense object will not be projected (failing to provide a true 3-dimensional perspective). Volume rendering of CT data (Fig. 3) produces a true 3-dimensional model that can be rotated and manipulated. Currently, volume rendering can be painstaking, although volume-rendering software may soon make such 3-dimensional reconstructions a part of standard CT interpretation, improving the study until it someday replaces the need for catheter angiography.9
Iain D.C. Kirkpatrick Michael P. Meyers Department of Radiology University of Manitoba Health Sciences Centre Winnipeg, Man.
In this issue
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

