


Abstract
A novel formulary has been developed in Nova Scotia with the objective of providing quality treatment with needed medications at affordable cost.Creation of the formulary has involved collaboration among health care professionals, seniors, the Department of Health and pharmaceutical companies. This is the first Canadian formulary to use the Anatomic, Therapeutic, Chemical system. Drug listing is comprehensive rather than exclusive. Colour-coded recommendations on use assist physicians with drug choice. Relative costs are indicated within each therapeutic grouping. Listings indicate drugs approved for reimbursement, interchangeable medications, maximum allowable cost, drug identification number and manufacturer code. Treatment summaries provide brief overviews of therapeutic advice. Updates on new products and new or modified treatment summaries are provided every 6 months. The formulary will be the focus of coordinate educational activities on treatment for seniors and health care professionals.
Opportunities for reform in Pharmacare in Canada include education of the public, pharmacists and physicians about drugs and therapeutics, enhanced cooperation and collaboration among seniors, pharmacists and physicians on better use of medications, and the development of new formularies to replace existing Pharmacare drug lists.
Many physicians view existing provincial drug lists as restrictive and, consequently, have a negative overall perspective of their place in pharmacotherapeutics. However, the ideal formulary should assist the physician in making optimal therapeutic decisions in symptom and disease management. When developed with a focus on excellence in patient care and with a collegial rather than an adversarial approach among the relevant stakeholders, the formulary should be a valuable aid to the complex process of prescribing the most cost-effective treatments. Furthermore, an effective formulary should empower patients, pharmacists and physicians to work together for quality treatment with needed medications, whether the payer is an individual, an insurance company or a provincial government.
Others with a need to be involved in the acceptance and dissemination of the formulary include professional associations of pharmacists and physicians, a representative of senior recipients of drug therapy, university faculty, the drug information service, the pharmaceutical manufacturers and those with direct or indirect responsibilities for financing the systems. Participation in the Nova Scotia Formulary Working Group included all these constituencies.
Elements of the Nova Scotia formulary
The Nova Scotia formulary is also novel in that it contains the following elements: Anatomical, Therapeutic, Chemical (ATC) system; comprehensive listing of drugs; recommendation on use (colour coding); relative cost (within the therapeutic grouping); interchangeable drugs; drugs with maximum allowable cost; drugs approved for reimbursement; drug identification number; manufacturer code; and treatment summaries.
Anatomical, Therapeutic, Chemical system
The ATC system was developed in Scandinavia for the study of pharmacoepidemiology. The system was adopted by the World Health Organization Pharmacoepidemiology Program and was subsequently introduced in Canada as a mechanism to facilitate therapeutic comparisons by the federal Patented Medicines Price Review Board. Two aspects of the ATC system are particularly appealing: the fact that prescribing is directed by disease within particular anatomic systems rather than classifications based on pharmacologic actions, and the proven value of the system in pharmacoepidemiologic research.
The ATC system has a branching logic that is intuitive with the therapeutic process. It begins with the anatomic system within which the disease or symptom occurs (e.g., cardiovascular system, angina pectoris), moves into the broad therapeutic category (antianginal) and, finally, provides specific chemical products that are of proven value in this setting (nitrates, beta-blockers and calcium-channel blockers). In this example, the final category (level 5) is the specific nitrate, beta-blocker or calcium-channel blocker that the physician may wish to prescribe.
Comprehensive listing of drugs
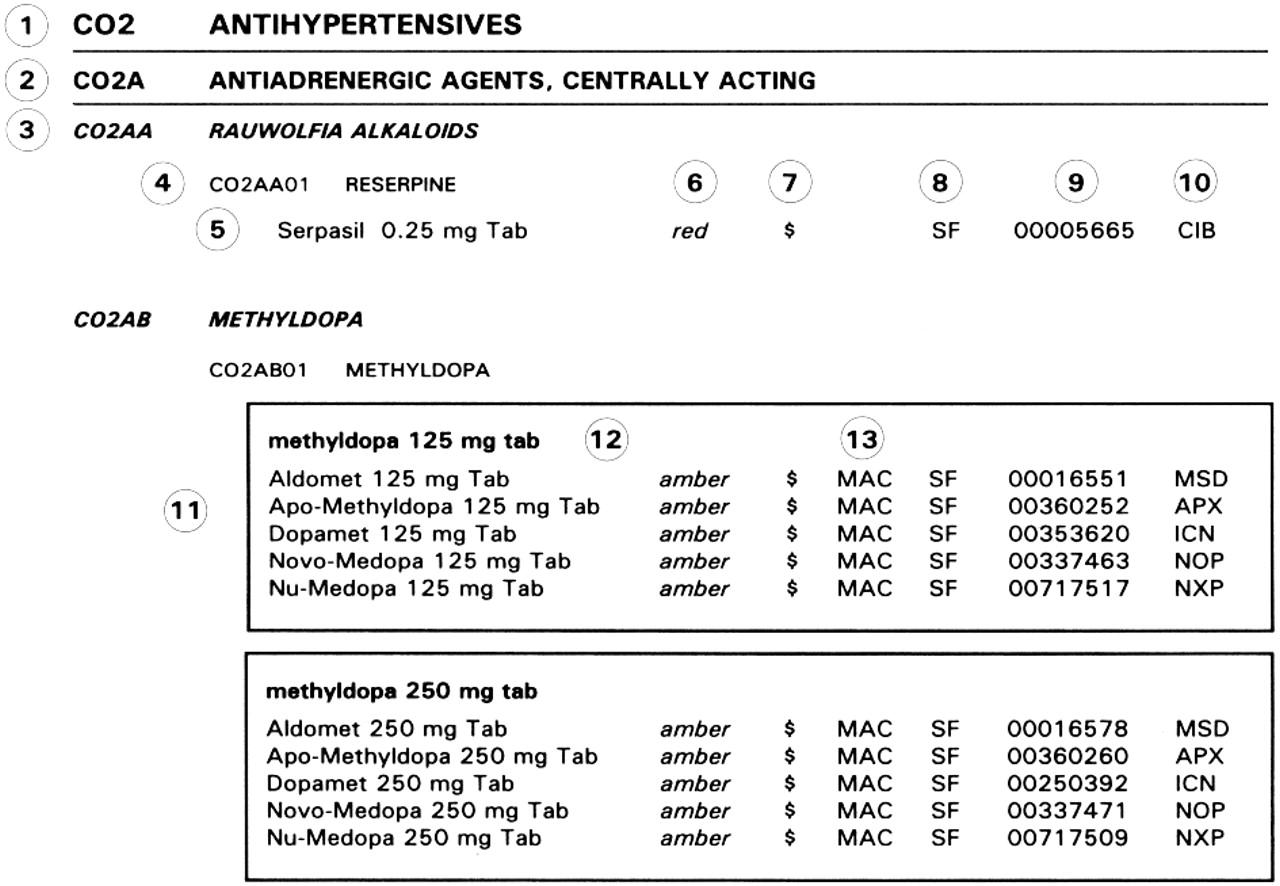
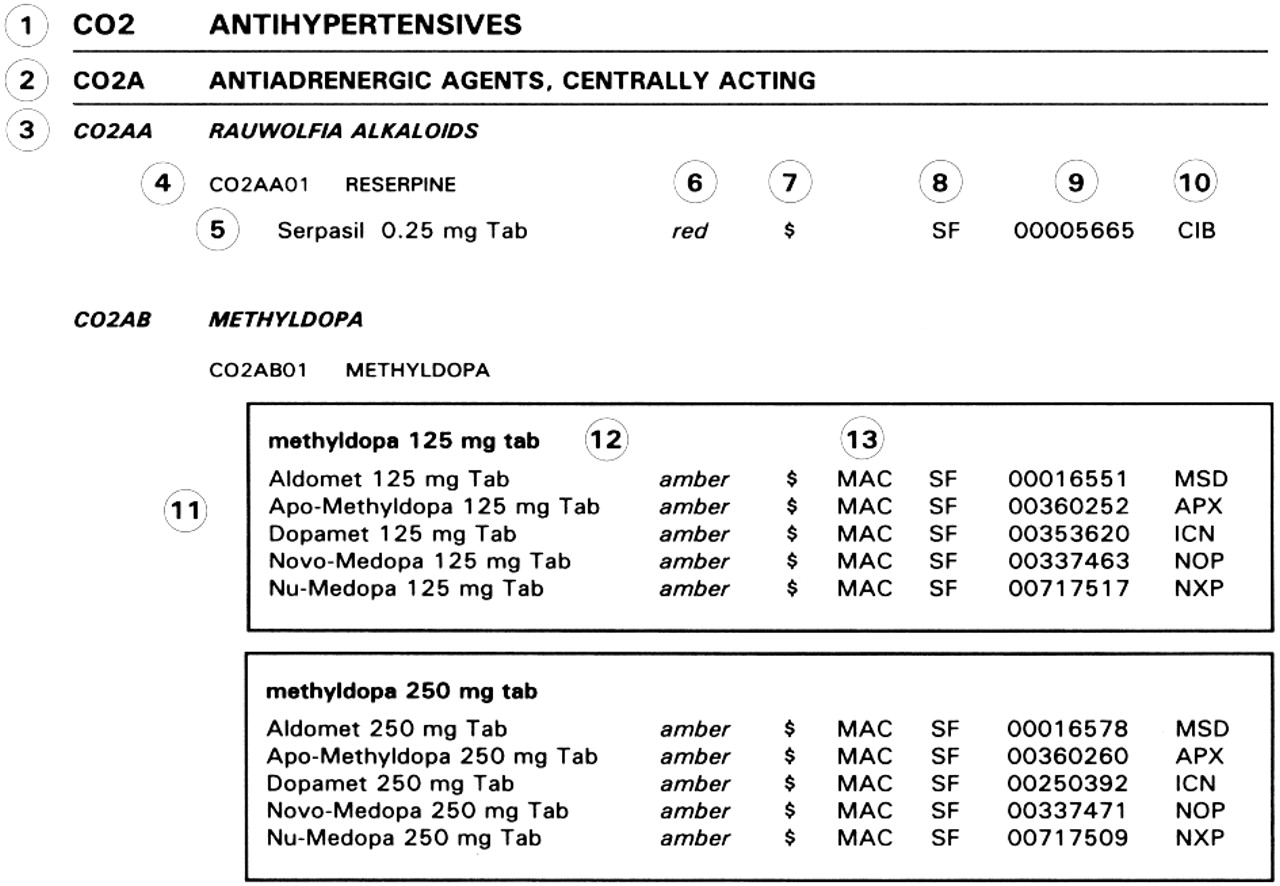
A comprehensive listing of drugs was decided on rather than an exclusive listing of drugs reimbursed under the program. An example of a listing is provided to assist the reader with the formulary layout (Figure 1).
{kind=link}
Figure 1. Example of a listing in the Nova Scotia formulary. 1 = therapeutic main group; 2 = therapeutic subgroup; 3 = chemical/therapeutic subgroup; 4 = subgroup for chemical substance; 5 = brand or manufacturer's name of the drug, including dosage form, or route and strength, or both; 6 = recommendation on use; 7 = relative cost; 8 = benefit status (plans for which the drug is a benefit); 9 = drug identification number; 10 = manufacturer code; 11 = interchangeable drug group box; 12 = interchangeable drug heading; and 13 = maximum allowable cost applies (if this column is blank, there is no maximum allowable cost).
Recommendation on use (colour coding)
To assist physicians in selecting the most appropriate therapy, a recommendation on use has been assigned to each product in a category. Therapeutic considerations, based on the recommendations in the treatment summaries rather than on costs, are the basis for classification as green, number or red. Older, established medications coded green or amber should not be abandoned for newer medications coded green or amber unless efficacy is substantially improved, toxicity is reduced, or cost-effectiveness is enhanced.
Green: These drugs are, for most indications, the first-line choice for treatment based on efficacy, safety and clinical experience.
Amber: These drugs are, for most indications, the second-line choice for treatment based on efficacy, safety and clinical experience.
Red: These drugs are, for most indications, the third-line choice for treatment based on efficacy, safety and clinical experience. Medications coded as red may require special expertise to determine use or to monitor therapy because of high risk of adverse effects or toxicity, or may be inappropriate compared with other agents that have similar therapeutic effects. As well, all drugs for intravenous use have been listed as red because they are generally administered in the hospital setting or at home by specially trained professionals.
In general, drugs designated as green or amber can be considered appropriate for physicians with general knowledge or experience of their use. Drugs designated as red should be used only be physicians with special expertise, and in many cases they require special written authorization. It was appreciated that this colour coding is somewhat arbitrary and that revision will likely be necessary as new information becomes available on the therapeutic value and relative toxicity of specific products.
Given a choice within a particular therapeutic category, and given a variety of options within a specific recommendation on use, whether it be green, amber or red, it is hoped that the physician will choose the least expensive product of those appropriate to treat a given patient. If the physician chooses a drug other than one designated green in the least expensive category, it is expected that she or he will be able to provide reasonable justification to the patient, the insurance company or the government payer for selecting an alternative product. Usual reasons are likely to be categorized as absolute (or relative) contraindication, development of a troublesome or serious adverse event, or failure to respond appropriately to a reasonable dosage and duration of treatment.
Relative cost (within each therapeutic grouping)
Drug within categories are compared in relation to the unit cost, daily cost and, in some instances, treatment costs. They are assigned 1, 2 or 3 dollar signs. Those coded $ are the least expensive, those coded $$ are moderately expensive, and those coded $$$ are the most expensive relative to other treatments used for similar therapeutic indications.
Interchangeable drugs
The formulary indicates drugs that have been deemed interchangeable by the Drugs and Therapeutics Committee of the Nova Scotia Department of Health.
Drugs with maximum allowable cost
For genetic drugs that meet the criteria for interchangeability, the Seniors and Family Benefits Pharmacare programs implemented the MAC program. This program sets a maximum allowable cost (MAC) for each interchangeable category with benefit status, based on the lowest-priced brand within that category. The additional cost of a higher-priced brand (usually the brand-name product) is paid by the patient. In the case of a documented adverse reaction to a particular brand, exceptions can be made to cover the cost of a more expensive drug.
"Special MACs" have been assigned to products relative to others within the same therapeutic classification. For example, the special MAC for the H2-receptor antagonists famotidine (Pepcid) and nizatidine (Axid) corresponds to an equivalent dose of ranitidine (Zantac). Again, the patient is required to pay the difference when a more expensive product is prescribed, unless the need for an exception is defined.
Drugs approved for reimbursement
Drugs are approved for reimbursement under 2 programs, of which the Seniors' program is the largest, accounting for 80% of the government's expenditure on Pharmacare. The benefit status of medications reimbursed under these programs is indicated by the letter S (Seniors' Pharmacare), F (Family Benefits and Income Assistance), D (Diabetic Assistance) or E (exception status drug). If this column is blank, the product is not a benefit under any of these programs.
Drug identification number and manufacturer
In keeping with standard formulary practice, the drug identification number and the standard manufacturer code are listed for each product.
Treatment summaries
Treatment summaries are brief overviews of therapeutic advice for prescribers. They are written by experts, edited and revised in collaboration with pharmacists who have special expertise in drug information, and updated as important new information on disease management is introduced. Relevant nonpharmacologic management is emphasized, in addition to a recommended approach to disease or symptom management with medications.
Format and updating
The formulary is presented in a loose-leaf binder in which drugs are divided by ATC classification. There are 2 indices. An alphabetical listing of drugs (both proprietary and nonproprietary names) directs the prescriber to the relevant ATC section. An alphabetical listing of treatment summaries is cross-referenced with the relevant ATC section. Routine updates for the formulary are provided at least every 6 months. Amendments include the addition of new drugs, additions to the lists of approved interchangeable products, deletions, alterations to colour coding, and new or modified treatment summaries. An electronic format of the formulary is being developed and will be made available to prescribers.
Discussion
Physicians are not expected to refer to the formulary in each therapeutic situation. Rather, it is expected that they will refer from time to time to the sections in the formulary that are relevant for the majority of their practice and that they will conduct informal self-audit and modify their usual prescribing practice accordingly. If the physician has reason to prescribe for a problem that is less familiar, the formulary should provide reasonably convenient access to needed information.
Individual physicians will receive an analysis of their prescribing habits that will enable them to compare their prescribing patterns with those of their peers by drug category and costs.
The bulkiness and weight of the paper document are barriers to the effective use of the formulary. The benefits of regular updating are partially offset by the time and inconvenience of exchanging parts of the earlier document with replacement pages and new additions. Accessibility of the latest formulary materials through computer networking is an important long-term goal. In addition, it is hoped that therapeutic guidelines and the formulary may ultimately be linked to the care of individual patients in electronic format.
The recommendation from the National Forum on Health that there be a Canadian Pharmacare system creates a challenge for each Canadian province and territory to develop a formulary consistent with the principles of the Canada Health Act. The framework of the Nova Scotia formulary is offered as a possible starting point for a "national" formulary, with the expectation that individual provinces and territories will have greater or lesser capacity to accept the financial implications of a national Pharmacare system.
Although concern had been expressed about the wisdom of including in the Nova Scotia Formulary Working Group representatives of pharmaceutical sectors whose philosophies and opinions often run contrary to each other, the industry representatives provided valued input and exemplified the same high level of purpose and collegiality as other members of the working group.
The adoption of a comprehensive listing of drugs coupled with the colour coding of recommendations and the inclusion of government funding policies likely avoided confrontations that may arise with an exclusive listing. This approach likely avoided the problems of interfering with the usual marketplace among manufacturers of similar medications, thereby enabling competition that may ultimately be beneficial to the consumer.
Through discussions and collaboration with the private insurance sector, it is possible to develop an entirely privately operated but government-sponsored system, an entirely government-sponsored and government-operated system, or a mixed government/private sector system, such as that introduced in Quebec. There is a need for greater uniformity in formulary development, even if the barriers to national Pharmacare preclude the realization of such a system in Canada.
I thank my colleagues in the Nova Scotia Formulary Working Group for their collaboration: Tim Dean, Deputy Chair; Carolyn Hatcher and Susan Radford, Nova Scotia Medical Services Insurance; Dawn Frail, Nova Scotia Department of Health; Anne Marie Whelan, College of Pharmacy, Dalhousie University; Gobin Sawh, Nova Scotia Senior Citizens' Secretariat; John Burgess, Pharmacy Association of Nova Scotia; Paul Renault, Medical Society of Nova Scotia; Brian Tuttle, Drug Information Centre, Camp Hill Medical Centre; Wayne Putnam, Department of Family Medicine, Dalhousie University; Julie Tam, Canadian Drug Manufacturers Association; and Anne Tomalin, Pharmaceutical Manufacturers Association of Canada. The outstanding support and assistance of Eleanor Hubbard and Emily Somers, of the Nova Scotia Department of Health, are greatly appreciated.
I take entire responsibility for the opinions expressed.
Competing interests: None declared.
This article has been peer reviewed.
Reprint requests to: Dr. S. George Carruthers, Rm. N587, Victoria Campus, London Health Sciences Centre, London ON N6A 4G5; fax 519 667-6626; [email protected]
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

