


Reason for posting: Serotonin syndrome is a rare but serious and sometimes fatal toxidrome characterized by mental, autonomic and neurologic symptoms.
Serotonergic psychotropic medications, including many antidepressants, have long been known to trigger the condition. The US FDA1 has now reported the condition in a number of people taking triptans concurrently with some antidepressants, particularly selective serotonin and serotonin– norepinephrine reuptake inhibitors (SSRIs and SNRIs, respectively).
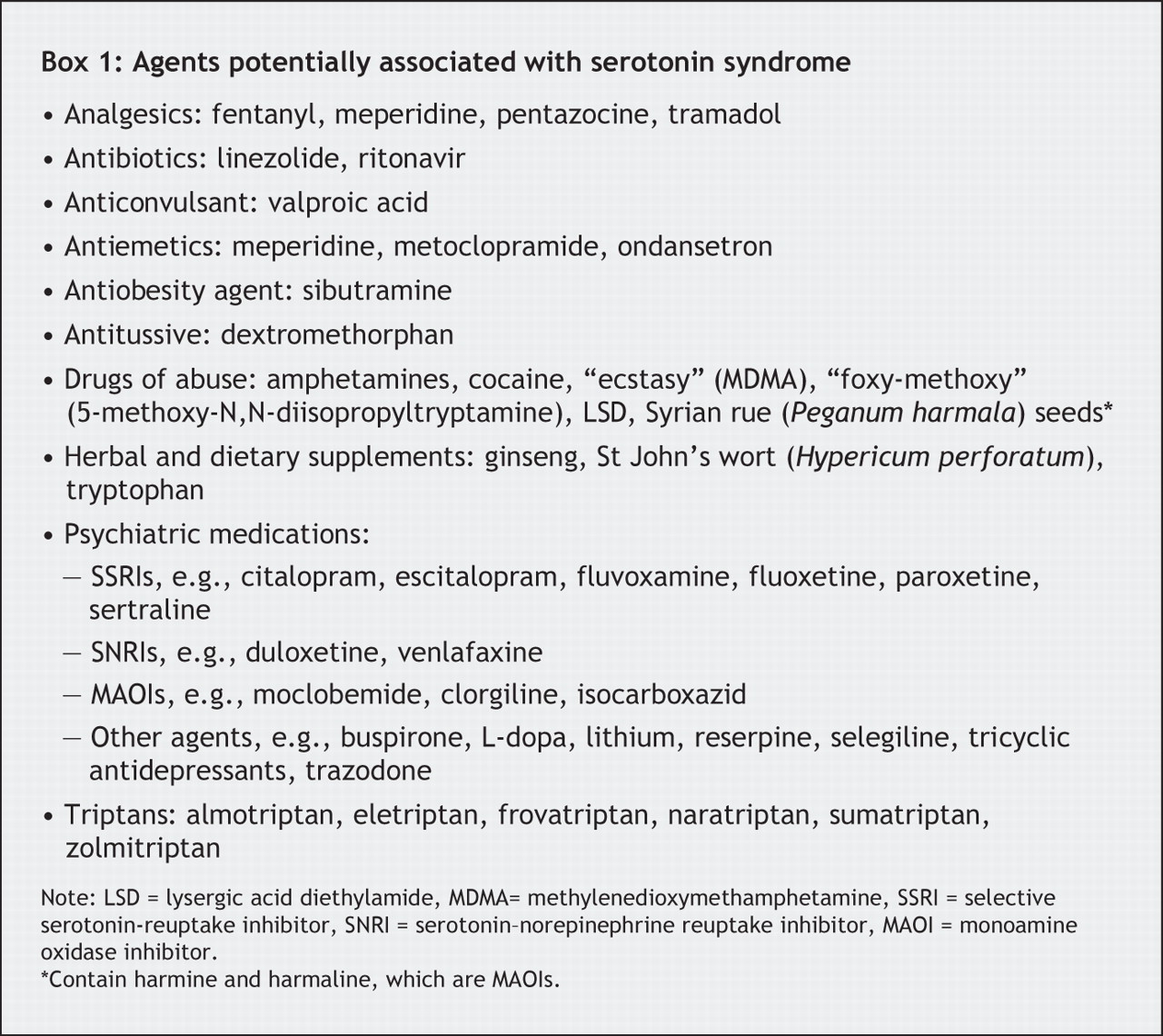
The drugs: Triptans are used intermittently to abort migraines. They act as selective 5-HT1B and 5-HT1D receptor agonists and lead to cranial vasoconstriction and neuronal inhibition. Along with triptans, a variety of agents (taken alone or in combination) can precipitate serotonin syndrome (Box 1).2–4 The pathophysiology of the condition appears to relate to increased serotonin synthesis (L-tryptophan) or to altered serotonin release, reuptake, catabolism or receptor agonism.3 The reasons for individual susceptibilities are still unclear. About 1 in 7 patients who overdose on antidepressants experience the syndrome.2

The symptoms of serotonin syndrome (Box 2)2–5 often have a rapid onset, usually within hours of the initiation or dose change of a drug, but occasionally up to several weeks after. Of note, serotonin syndrome can appear as a mild case in which the patient is afebrile but shivers and experiences no other symptoms beyond tachycardia, diaphoresis, mydriasis, tremor and myoclonus.2

No diagnostic test is specific for the condition, but laboratory abnormalities often include metabolic acidosis, elevated muscle enzymes (creatinine phosphokinase, alanine and aspartate aminotransferases, lactic dehydrogenase) and creatinine, disseminated intravascular coagulopathy, leukocytosis and ventricular arrhythmia.2–4
The FDA is aware of 27 cases involving patients taking SSRIs or SNRIs and triptans. In 2 cases, the patients' life was endangered; 13 of the 27 patients were admitted to hospital. Many of these patients had taken the drugs in combination previously, without problems. In 8 cases, recent dose increases or the addition of another serotonergic drug to an SSRI– triptan or SNRI– triptan combination were related to symptom onset, which occurred a median of 1 day (range 10 minutes to 6 days) afterward.1
What to do: Triptans and antidepressants are widely prescribed and have a biologically plausible interaction. Although the risk of serotonin syndrome appears to be low, prescribers of either class of medications should ask patients about medications prescribed elsewhere, to discover any that may interact. Users of triptan in combination with an SSRI or SNRI should be warned of this rare but serious adverse effect. During periods of drug initiation, dose escalation or the addition of another serotonergic agent, patients should be particularly vigilant for symptoms of concern (Box 2) and seek urgent medical attention if any occur. The offending agents should be withdrawn, and patients closely monitored and treated with supportive measures as required.4

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

