


A 71-year-old woman was assessed before undergoing a vaginal hysterectomy, bilateral salpingo-oophrectomy and pelvic lymph node dissection for stage I endometrial cancer. She had experienced a spontaneous subarachnoid hemorrhage in 2005, with no residual deficits, and had hypertension and osteoarthritis of the knee. She had no functional limitations, no signs or symptoms of heart failure, no chest pain or previous diagnosis of coronary artery disease, and no history of diabetes mellitus. Her blood pressure was well controlled with perindopril (2 mg daily). She was overweight (body mass index 28.7 kg/m2); otherwise, results from a physical examination were normal. Her creatinine level was within normal limits.
What preoperative investigations should be ordered for this patient?
Electrocardiogram (ECG)
Measurement of preoperative brain natriuretic peptide (BNP)
Chest radiograph
No testing required before surgery
The correct answer is (d). The 2016 guideline for perioperative risk assessment from the Canadian Cardiovascular Society recommends that patients requiring urgent or semiurgent surgeries without features on history or physical examination to suggest an unstable coronary syndrome or an obstructive intracardiac lesion should undergo surgery without further testing (d).1 Patients requiring emergent procedures should undergo surgery regardless of suspected cardiac disease.1 As this patient did not have signs or symptoms of cardiac disease, and her surgery was considered semiurgent (surgery for cancer with a potential to metastasize), she did not have testing before surgery.
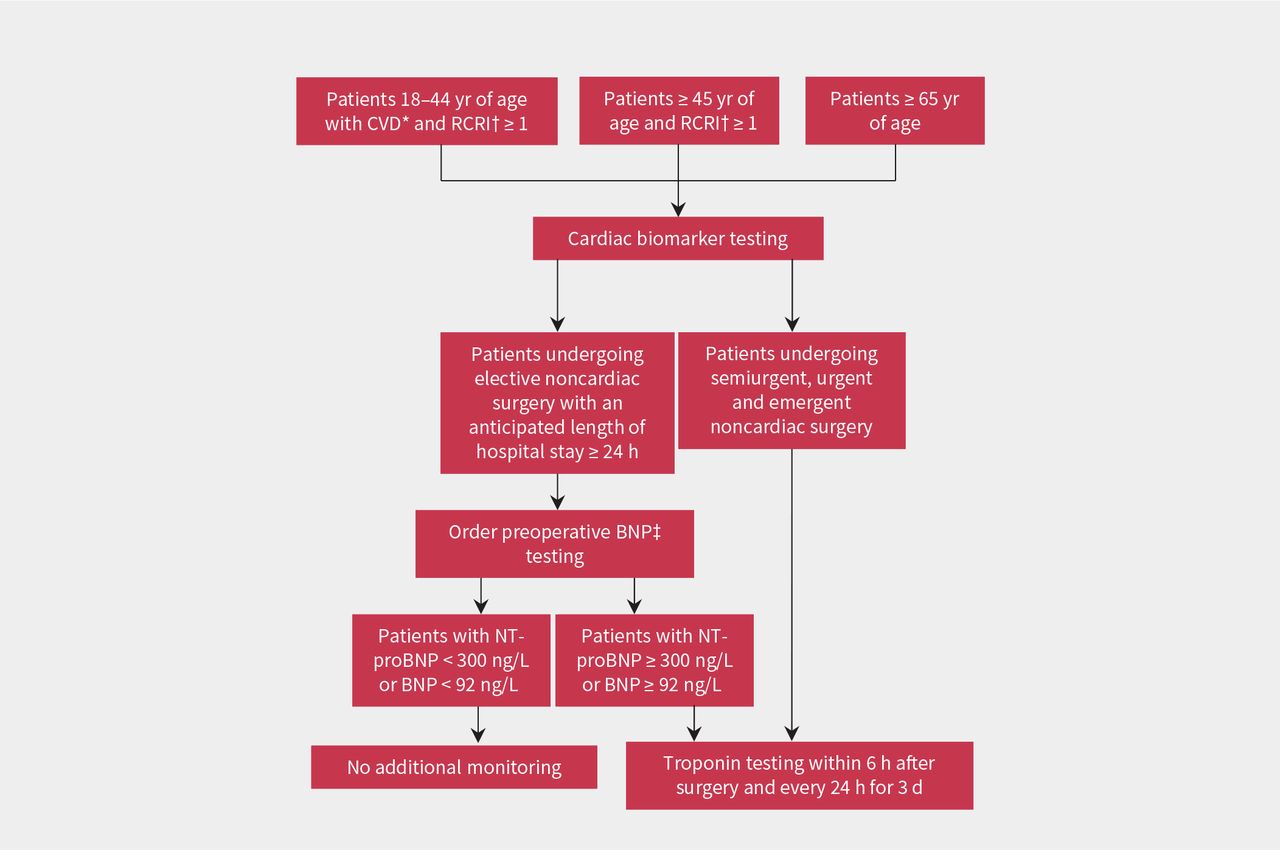
In patients undergoing elective surgery that requires an overnight admission to hospital, the society guideline recommends measurement of preoperative BNP (including the N-terminal fragment of proBNP or BNP) to predict cardiovascular complications in certain patients at high risk (b).1 Patients who are 65 years of age or older, those who are 45 years of age or older with a revised cardiac risk index of 1 or more, or those who are 18–44 years old who have vascular disease and a score of 1 or more are considered to be at high enough risk to warrant measurement of BNP (Figure 1).1 The revised cardiac risk index is a 6-point clinical risk score that assigns 1 point for each of coronary artery disease, congestive heart failure, cerebrovascular disease, diabetes mellitus requiring treatment with insulin, serum creatinine greater than 177 μmol/L or high-risk surgery2 (Box 1). Increasing scores correlate with higher postoperative risk of cardiac events and death.1,2 Patients who meet the above criteria who do not have preoperative BNP testing (including those who do not have BNP testing because they require emergent, urgent or semiurgent surgery) and those with elevated BNP levels should have postoperative troponin monitoring (Figure 1). Our patient was older than 65 years and had a score of 1 (for high-risk surgery); therefore, she qualified for postoperative troponin measurement.
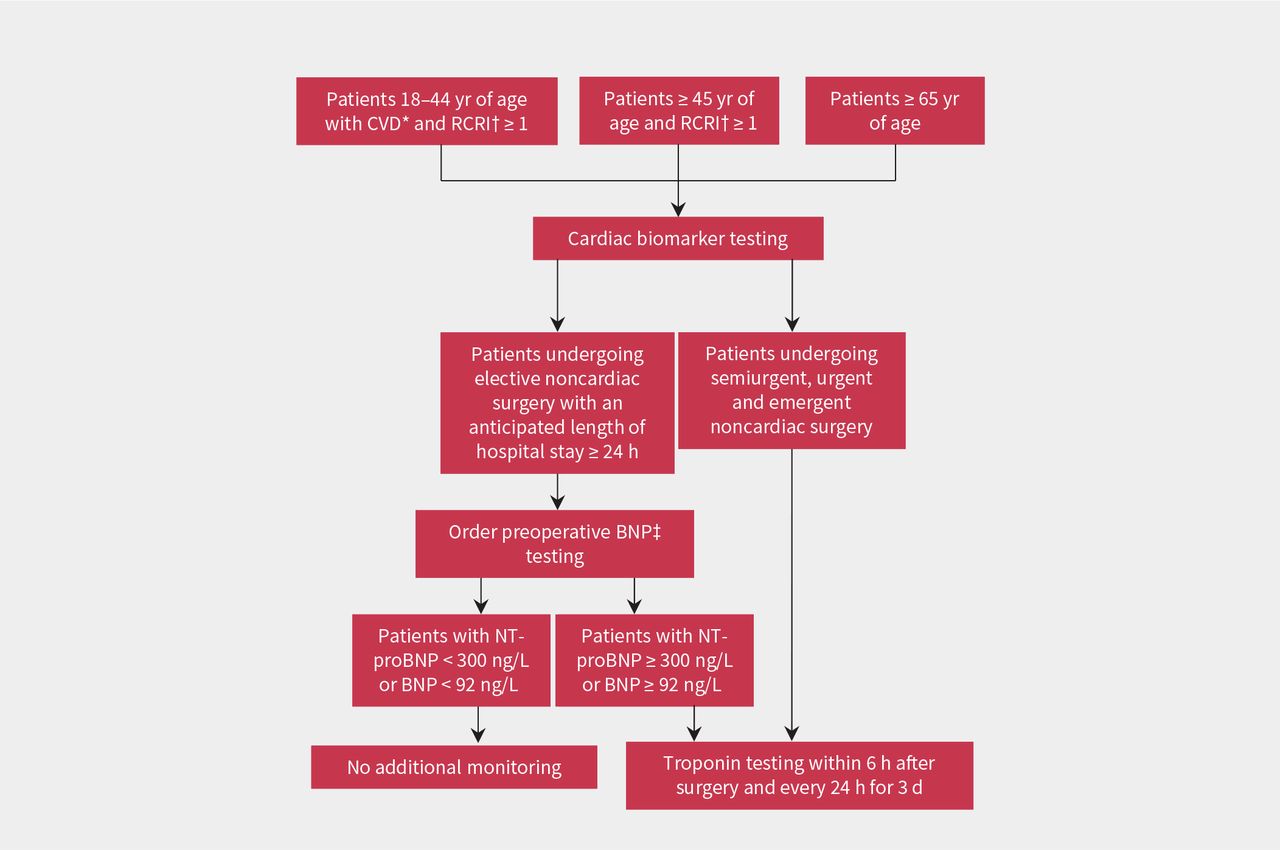
Canadian Cardiovascular Society recommendations for perioperative cardiac risk assessment in adult patients undergoing elective noncardiac surgery with an anticipated inpatient hospital admission longer than 24 hours.1 Note: BNP = brain natriuretic peptide, CVD = cardiovascular disease, RCRI = revised cardiac risk index. *Includes coronary artery disease, cerebrovascular disease, peripheral arterial disease, congestive heart failure, pulmonary hypertension or severe obstructive intracardiac abnormality (e.g., severe aortic or mitral stenosis). †Revised cardiac risk index assigns 1 point for each of high-risk surgery (intraperitoneal, intrathoracic or superinguinal vascular surgery), coronary artery disease, congestive heart failure, cerebrovascular disease, diabetes mellitus on insulin therapy or serum creatinine level > 177 μmol/L (Box 1). ‡Refers to N-terminal (NT) fragment of proBNP or BNP.
| RCRI criteria | Definition |
|---|---|
| History of ischemic heart disease | History of myocardial infarction, positive exercise stress test, current report of angina, current nitrate use or ECG with pathologic Q waves |
| History of congestive heart failure | History of congestive heart failure, pulmonary edema or paroxysmal nocturnal dyspnea, or physical examination showing bilateral rales or S3 gallop, or chest radiograph showing pulmonary vascular redistribution |
| History of cerebrovascular disease | History of transient ischemic attack or stroke |
| Diabetes mellitus with insulin use | |
| Preoperative serum creatinine ≥ 177 μmol | |
| High-risk surgery | Intraperitoneal, suprainguinal vascular or intrathoracic surgery |
Note: ECG = electrocardiography, RCRI = revised cardiac risk index.
* The RCRI is a 6-point clinical risk score that assigns 1 point for each of the criteria listed above.2
Increasing scores correlate with higher postoperative risk of cardiac events and death.1,2
Choosing Wisely Canada recommends against preoperative ECG (a) in asymptomatic patients undergoing noncardiac surgeries, based on evidence that ECGs do not improve preoperative risk stratification and often lead to additional, low-benefit testing. 3 Our patient was asymptomatic and did not have a clear preoperative indication for an ECG. Choosing Wisely Canada also recommends against baseline radiographs of the chest (c) in asymptomatic patients preoperatively because of a high rate of false-positive results.3
We ordered troponin testing for our patient on the first, second and third days after surgery. On postoperative day 1, her serum high-sensitivity troponin T was 50 (normal less than 14) ng/L, which rose to 87 ng/L and then 119 ng/L on serial assessments. Her ECG (Figure 2) and vital signs were normal. She had no chest pain or pressure, nausea, dyspnea or palpitations. A repeat physical examination showed no changes.

Postoperative electrocardiogram for a 71-year-old woman with elevated troponin, showing no features of ischemia.
What is the most likely diagnosis?
Unstable angina
Non-ST-segment elevation myocardial infarction (non-STEMI)
Myocardial injury after noncardiac surgery
Pulmonary embolism
Our patient met the diagnostic criteria for myocardial injury after noncardiac surgery (c), defined by a postoperative rise in serum troponin that is not attributable to another cause such as sepsis4 (Box 2). Using the high-sensitivity troponin T assay, myocardial injury after noncardiac surgery can be diagnosed when the absolute value is greater than 65 ng/L or between 20 and 64 ng/L and rising by 5 ng/L on serial measurements. Myocardial injury after noncardiac surgery can also be diagnosed using a non–high-sensitivity troponin assay (Box 2). This condition is found in about 17% of patients at high risk after noncardiac surgery and is associated with a 2.7-fold increased risk of death in the first 30 days after surgery.4 Between 80% and 90% of patients with myocardial injury after noncardiac surgery are asymptomatic and are detected only with troponin surveillance.4,7
| Assay | Threshold for MINS | 30-d mortality, % |
|---|---|---|
| High-sensitivity troponin | 20–65 ng/L and rising by 5 ng/L | 3.0 |
| ≥ 65 ng/L | 9.1 | |
| Troponin T | ≥ 0.03 ng/mL | 9.8 |
| Other troponin assay | Greater than 99th percentile; 10% coefficient of variation | Unknown |
Note: MINS = myocardial injury after noncardiac surgery.
Although myocardial injury after noncardiac surgery includes patients with acute coronary syndromes if the diagnostic criteria for these events are also met, our patient did not have features consistent with acute coronary syndrome. Unstable angina (a) is diagnosed in patients with typical ischemic chest pain with normal troponin and ECGs. The diagnosis of non-STEMI (b) requires ischemic symptoms or ECG changes. Pulmonary embolism (d) is an important diagnosis in the postoperative period but does not typically present with asymptomatic troponin elevation.
What is the next step in management of this patient?
Coronary angiography
Computed tomography (CT) of the chest with pulmonary embolism protocol
Initiation of acetylsalicylic acid (ASA) and statin therapy with comprehensive cardiac risk assessment
Pharmacologic cardiac stress testing
The Canadian Cardiovascular Society guideline recommends initiation of ASA and a statin in patients with myocardial injury after noncardiac surgery (c).1 This recommendation is based on data from an international prospective cohort study involving 415 patients that showed improved survival in patients with myocardial injury after noncardiac surgery who were taking ASA and statins in the perioperative period.8,9 A recently reported randomized clinical trial7 found that dabigatran reduced major vascular complications in patients with myocardial injury after noncardiac surgery without a significant reduction in mortality; however, these data were published after the most recent society guideline was released.1,7 To our knowledge, this latter management strategy has yet to be widely adopted.
Although it is probable that patients with myocardial injury after noncardiac surgery have underlying, unrecognized coronary artery disease, neither coronary angiography (a) nor stress testing (d) is currently recommended in patients with myocardial injury after noncardiac surgery in the absence of other features or symptoms. Although pulmonary embolism is an important complication in the postoperative period, CT of the chest with pulmonary embolism protocol (b) is indicated only if symptoms or signs of pulmonary embolism are present.
We prescribed atorvastatin (40 mg at bedtime) and ASA (81 mg daily). We restarted perindopril and increased the dosage to 4 mg once daily. The patient was seen at the outpatient internal medicine follow-up clinic 30 days after discharge. Her glycated hemoglobin A1c was normal. She reported episodes of palpitations, and an ECG showed frequent premature ventricular complexes. Because of these new symptoms, we ordered a myocardial perfusion imaging scan, which showed a moderate volume of ischemia in the area of the left anterior descending artery, with normal left ventricular systolic function.
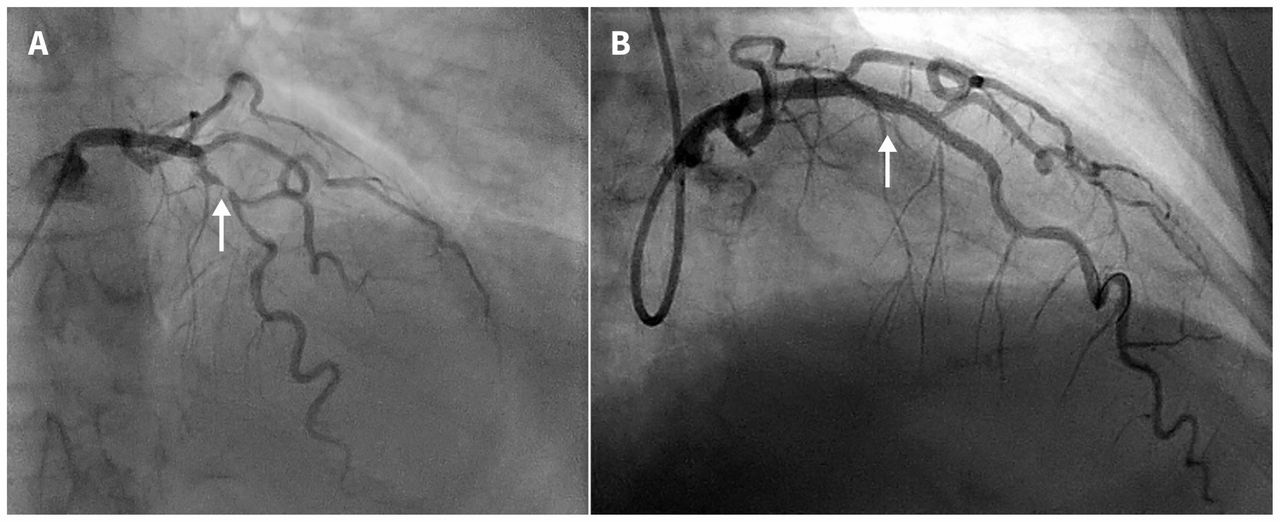
Our patient underwent coronary angiography that showed a diffuse 90% mid-left anterior descending artery lesion (Figure 3). She underwent percutaneous coronary intervention with a drug-eluting stent. We prescribed dual antiplatelet therapy and referred her for cardiac rehabilitation therapy. The patient was well at six-month follow-up.

Cardiac angiogram for the patient showing the 90% mid-left anterior descending artery lesion (A) before and (B) after percutaneous coronary intervention with a drug-eluting stent.
Discussion
There are nearly 500 000 noncardiac surgeries performed in Canada each year.10 The mortality rate for adults undergoing elective, noncardiac surgery is 1.2%, and increases in patients who have postoperative increases in serum troponin (Box 2).4,7 Myocardial injury after noncardiac surgery, defined as an elevation of troponin level to greater than the 99th percentile of normal, is a recently recognized risk factor for death in the postoperative period.1
Management of patients at high risk in the perioperative period requires coordination of care between family physicians, internists, anesthesiologists and surgeons. Surveillance using cardiac biomarkers is a new method for identifying patients at high-risk of perioperative complications. Patients with myocardial injury after noncardiac surgery are at high risk of short- and long-term cardiac events including death.4 Treatment begins with identifying these patients in the postoperative period using troponin screening, initiating long-term ASA and statin therapy and ensuring close clinical follow-up.
Recent evidence suggests that the use of dabigatran may have a role in reducing major vascular complications in myocardial injury after noncardiac surgery;7 however, interventions to reduce the high mortality rate observed in these patients have yet to be defined.
Footnotes
Competing interests: Kristin Lyons coauthored the 2016 Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery. No other competing interests were declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Contributors: Rahim Kachra conceived the work. Kristin Lyons and Shannon Ruzycki conducted the literature review. All of the authors wrote the manuscript and revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
In this issue
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

