


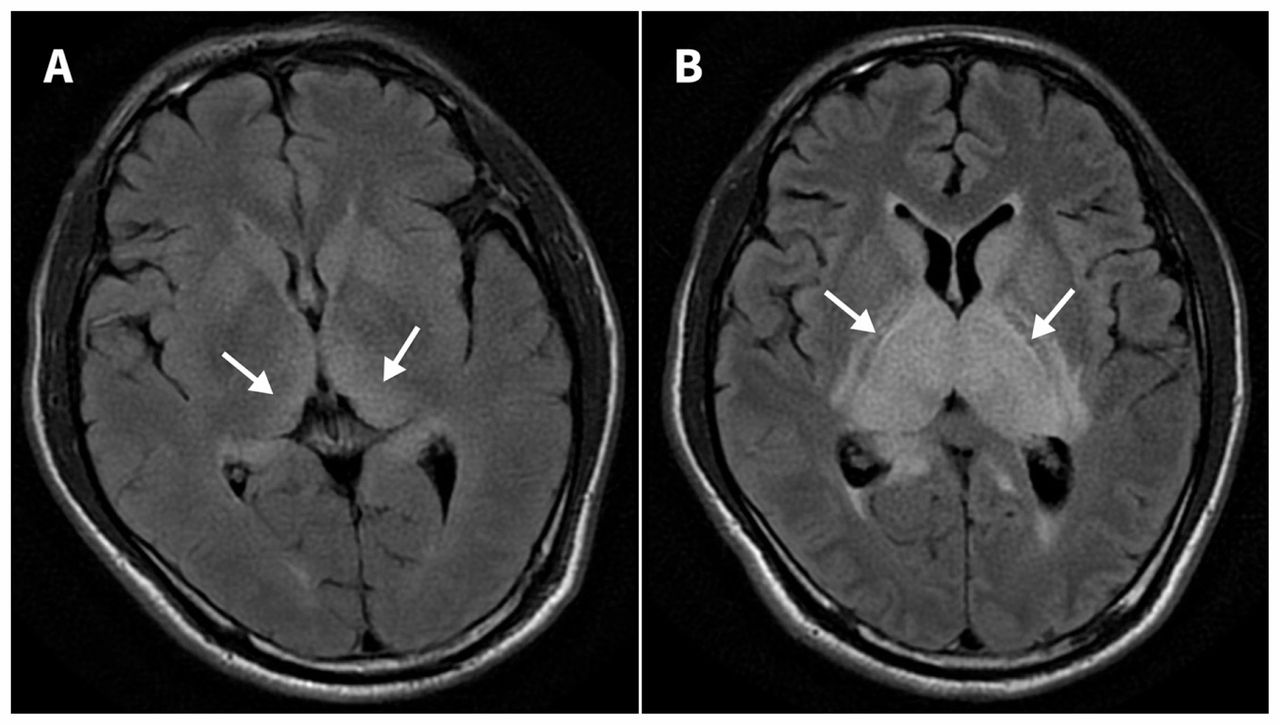
A previously healthy 52-year-old man was admitted with fever, headache and drowsiness of one day’s duration. He had neck stiffness and equivocal Kernig and Brudzinski signs. Cerebrospinal fluid showed an elevated protein level, a normal glucose concentration and lymphocytic pleocytosis. The patient’s mental status deteriorated on day 4. He became comatose and required mechanical ventilation. No intracranial hemorrhage was detected on brain computed tomography (CT). Serial brain magnetic resonance imaging (MRI) with fluid-attenuated inversion recovery sequence ( Figure 1A, on day 1, and Figure 1B, on day 5) showed progressively marked high signal intensities in the bilateral thalami (arrows), caudate nuclei and internal capsules. Diffusion-weighted MRI showed hyperintensity in the same area. There was no evidence of occlusion or high-grade stenosis of the basilar artery and main trunk of the bilateral posterior cerebral arteries. The finding was highly suggestive of Japanese encephalitis, and the diagnosis was confirmed later when the virus was detected in the cerebrospinal fluid by real-time reverse transcriptase polymerase chain reaction. Despite aggressive treatment with intravenous immunoglobulin and high-dose intravenous steroids, the patient died 30 days after admission.

(A) Brain magnetic resonance imaging (MRI) scan with fluid-attenuated inversion recovery (FLAIR) sequence on day 1 showing mildly high signal intensities in the bilateral thalami (arrows) in a 52-year-old man with Japanese encephalitis. (B) Brain MRI with FLAIR sequence on day 5 showing markedly high signal intensities in the bilateral thalami (arrows), caudate nuclei and internal capsules.
Japanese encephalitis virus, a mosquito-borne flavivirus, is the most common cause of viral encephalitis in Asia and the western Pacific rim. Although most of those infected are asymptomatic, 20%–30% of those who present with overt disease have fatal cases, and 30%–50% of survivors have neurologic, cognitive or behavioural sequelae.1 Clinical features include acute febrile illness, altered mental status, acute psychosis, seizure and acute flaccid paralysis. Thalamic abnormalities seen on imaging, such as hypodensity on CT and hyperintensity on T2-weighted MRI, have a high specificity for Japanese encephalitis in endemic areas.2 Although MRI is more sensitive than CT in detecting thalamic lesions in Japanese encephalitis,3 its diagnostic utility in the very early stage of the disease remains uncertain. Because of slowness to diagnosis, the reported mean duration between disease onset and MRI is about 10–20 days.2,3 The differential diagnosis includes metabolic diseases (e.g., hypoxic-ischemic encephalopathy, Wilson disease or Wernicke encephalopathy), vascular diseases (e.g., deep cerebral vein thrombosis or arterial occlusion), neoplasms (e.g., primary thalamic glioma) and flavivirus encephalitis other than Japanese encephalitis (e.g., West Nile fever and Murray Valley fever).4 The treatment for Japanese encephalitis remains supportive with no effective therapy.5
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained consent from the patient’s wife.
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

