


See also pages 485, 529, www.cmaj.ca/lookup/doi/10.1503/cmaj.151209 and www.cmaj.ca/lookup/doi/10.1503/cmaj.150550
A 62-year-old male smoker with hypercholesterolemia was admitted to the emergency department with substantial chest pain of 90 minutes’ duration. Electrocardiography (ECG) showed 1- to 2-mm upsloping ST-segment depression in the precordial leads, with tall and positive symmetric T waves, loss of precordial R-wave progression and small ST-segment elevation in the aVR lead (Figure 1). These ECG changes suggested de Winter syndrome, a condition associated with acute occlusion of the left anterior descending coronary artery and no ST-segment elevation. Urgent coronary angiography showed complete occlusion of the mid left anterior descending coronary artery, which was successfully treated with angioplasty and a drug-eluting stent (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150816/-/DC1). After angiography, the cardiac troponin I level rose to a peak of 85 μg/L. The patient had an unremarkable course after revascularization, with mildly depressed left ventricular ejection fraction, and was discharged after smoking-cessation and lifestyle counselling.

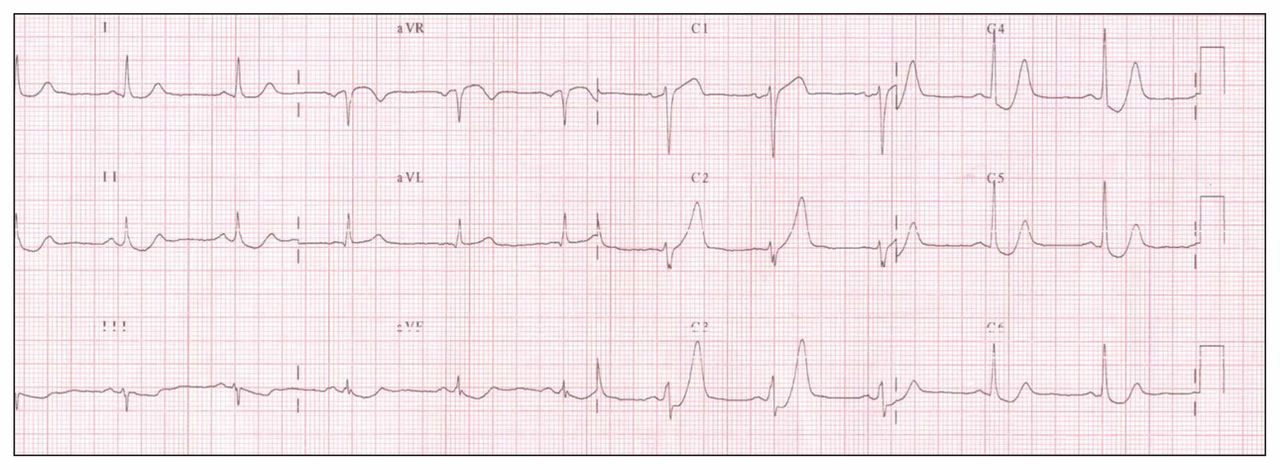
Electrocardiogram showing 1- to 2-mm upsloping ST-segment depression in the precordial leads of a 62-year-old man who presented with substantial chest pain, with tall and positive symmetric T waves, loss of precordial R-wave progression and small ST-segment elevation in the aVR lead.
Recognition of characteristic ECG changes associated with acute occlusion of a coronary artery guides decisions about reperfusion therapy. A current guideline defines ST-segment elevation myocardial infarction (STEMI) as a clinical syndrome characterized by typical symptoms of myocardial ischemia in association with persistent ST-segment elevation on ECG and subsequent release of biomarkers of myocardial necrosis.1 However, the same guideline recognizes that ECG abnormalities other than ST-segment elevation may indicate transmural myocardial injury.
We have described a patient with de Winter syndrome, a condition associated with typical chest pain and a characteristic ECG pattern without classic ST-segment elevation, yet acute total occlusion of the left anterior descending coronary artery. This syndrome is estimated to be present in about 2% of patients with acute anterior myocardial infarction2 but is under-recognized by clinicians and hence is associated with increased morbidity and mortality. Physicians, paramedics and others involved in the triage of patients with chest pain should be able to rapidly recognize this STEMI-equivalent ECG pattern to ensure appropriate, urgent reperfusion treatment.
Acknowledgement
The authors thank Philip Brabyn for English editing services.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

