


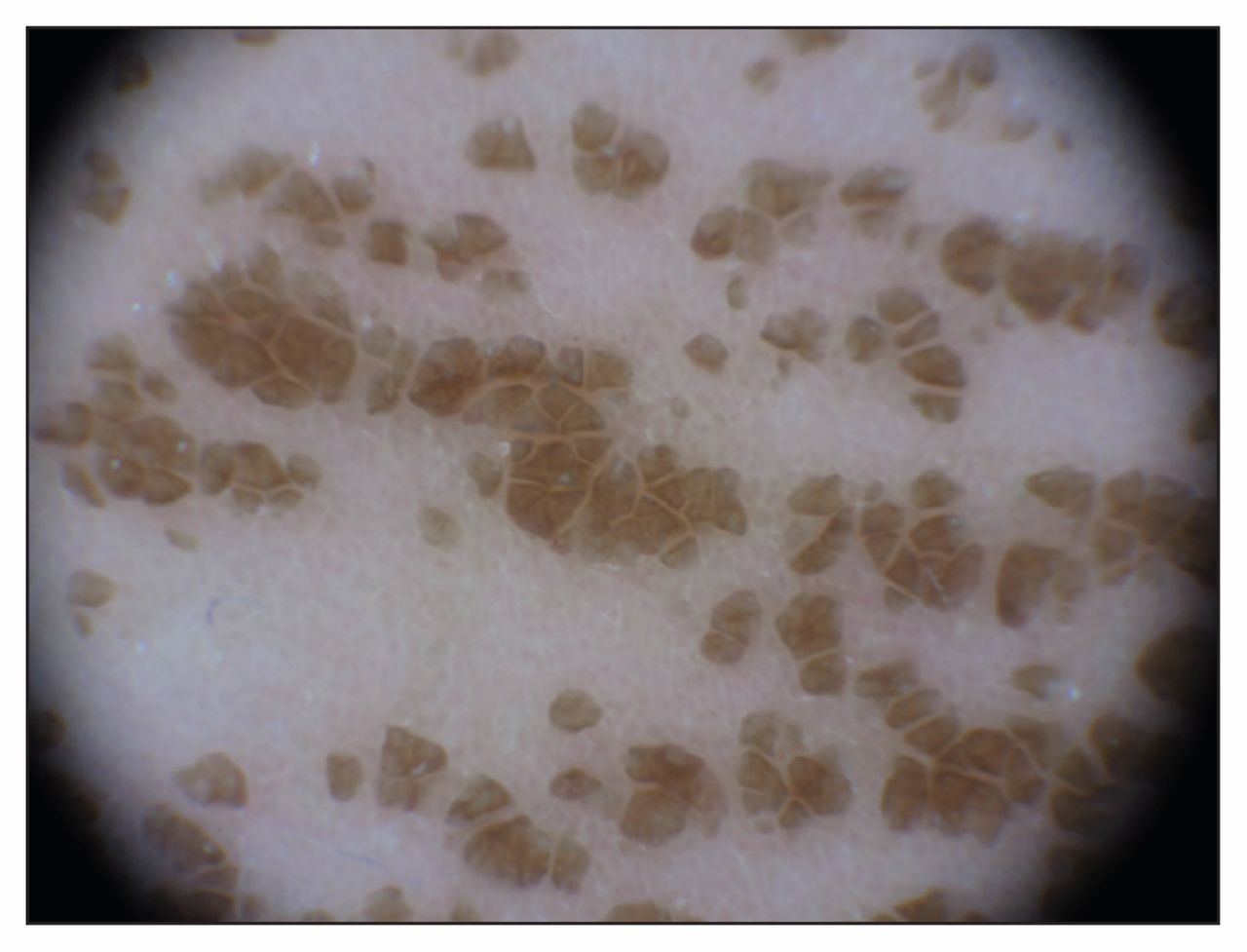
A seven-year-old girl was referred to our outpatient dermatology department with a six-month history of asymptomatic thin papillomatous brown plaques on her neck and the medial aspect of both arms (Figure 1A). The eruption had been treated by a general pediatrician as a mycotic infection with ketoconazole 2% cream twice daily for three months, with no response. Medical history was unremarkable. Dermoscopic examination showed polygonal areas of brownish pigmentation (Figure 2). Firm rubbing with a 70% isopropyl alcohol swab immediately caused the complete resolution of the plaques (Figure 1B).
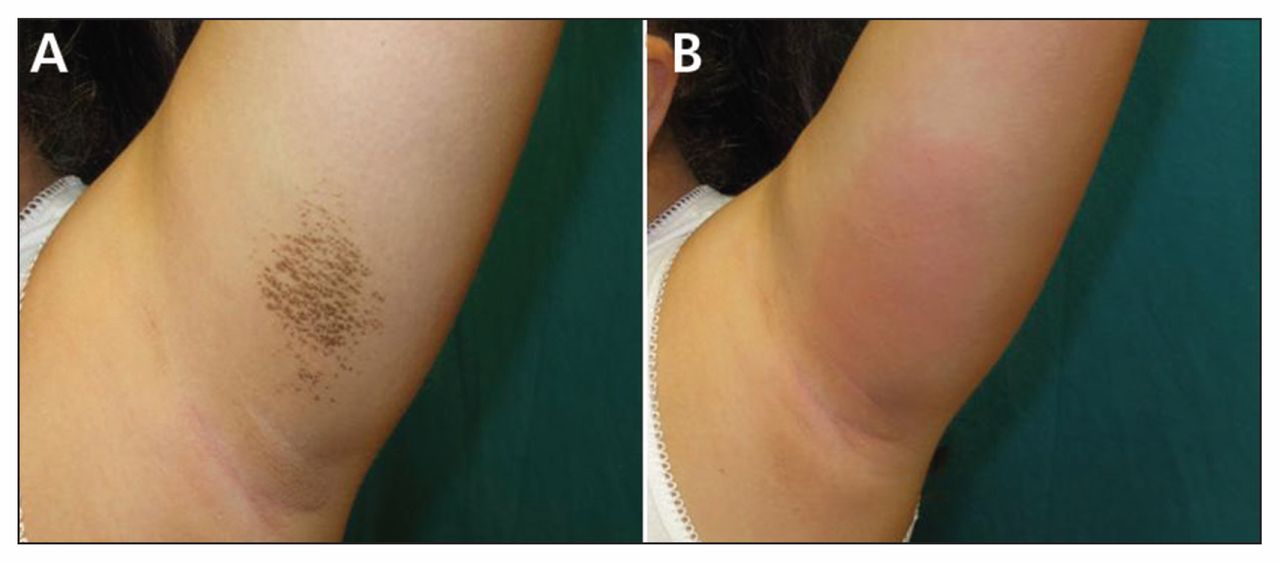
(A) Brown, dirt-like plaques on the left upper arm of a seven-year-old girl. (B) Complete resolution of the plaques after firm rubbing with 70% isopropyl alcohol.
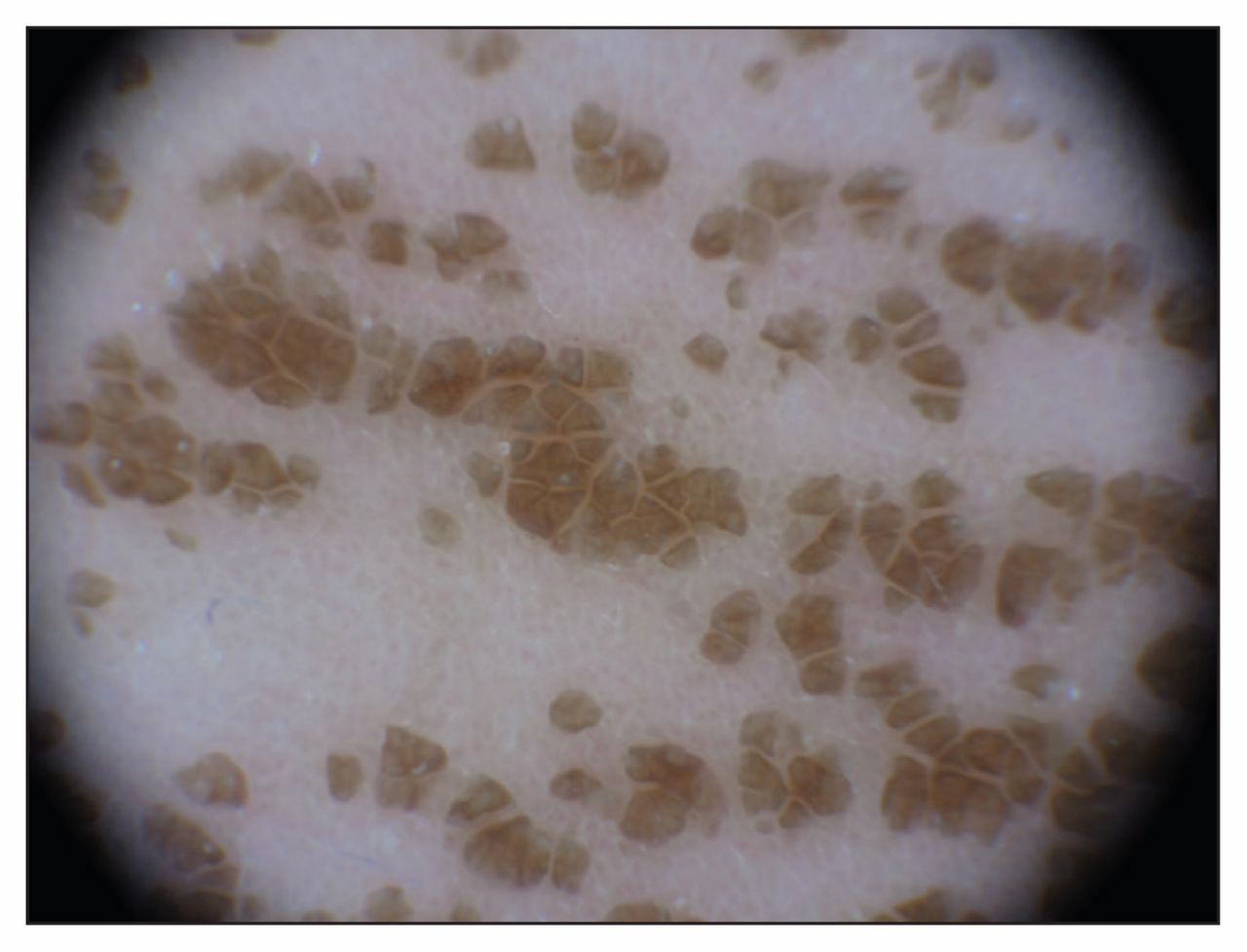
Dermoscopic image showing polygonal areas of brownish pigmentation.
Terra firma–forme dermatosis, also called “Duncan dirty dermatosis,” derives from Latin for “solid earth” and is often suspected based on its distinctive clinical presentation as a hyperpigmented dirt-like brown eruption on the skin. It is an idiopathic condition that affects mainly the pediatric population, though its incidence and prevalence have not been systematically estimated.1 Lesions may appear verrucous, reticulated and stuck-on, often affecting the neck, ankles and face. In contrast to patients with dermatitis neglecta, patients with terra firma–forme dermatosis typically have good hygiene habits. Vigorous but unsuccessful attempts at cleansing the affected areas are often described.
Pathologic examination usually is not necessary unless another condition is suspected, owing to the location or pattern of the lesions or clinical symptoms.2 The differential diagnosis, summarized in the algorithm proposed in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150075/-/DC1), includes conditions such as acanthosis nigricans, confluent and reticular papillomatosis, tinea versicolour and ichthyosis vulgaris.3 Dermoscopic examination may help narrow the differential diagnosis if a “stone pavement” pattern is observed, as in our patient. Resolution of the lesions after swabbing with 70% ethyl or isopropyl alcohol confirms the diagnosis.1
Terra firma–forme dermatosis can be treated with the diagnostic method itself, or with salicylic acid–based exfoliants and other keratolytic agents to accelerate the skin’s return to normal. Topical corticosteroids are not helpful in this condition.4
Acknowledgement
The authors thank the patient’s parents for providing permission to share her story.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

