


Wait times for bariatric surgery
Increasing rates of obesity have led to growing demand for bariatric surgery, a cost-effective treatment for severe obesity. How have wait times been affected? In this retrospective cohort study, researchers analyzed the impact of patient and operational factors on wait times for bariatric surgery at a tertiary care hospital in Toronto, Ontario. Of the 1664 patients referred for surgery between 2008 and 2011 who were included in the analysis, 724 underwent the procedure. Patients waited a mean of 440 (standard deviation 198) days, with a median wait time of 445 (interquartile range 298–533) days, far beyond the provincially mandated target of 365 days from referral to surgery. Some waited as long as 4 years, while others had surgery as soon as 3 months after referral. Nearly half the excess time was spent between referral and program orientation. Factors affecting wait times included active substance use and referral later in the study period. Body mass index, sex and distance from the hospital did not affect wait times (Table 1). The authors noted that previous operational decisions significantly increased the wait time for surgery and recommended that the implications of process-level decision-making be carefully considered before implementation. CMAJ Open 2015;3:E331–7.
Differences in time-to-surgery (only patients who underwent bariatric surgery were included in the analysis (n = 724)*
Sex differences in methadone maintenance treatment for opioid use disorder
Men and women differ in susceptibility to opioid use disorder, but they also differ in their response to methadone treatment. Using treatment standards that offer the same clinical management of this disorder for both men and women may not achieve optimum treatment outcomes for either sex. This systematic review included 20 studies (18 observational, 2 randomized clinical trials) that looked at sex differences in outcomes of methadone treatment, including drug use, health status and social functioning. Among the 9732 participants, women were less likely than men to use alcohol (odds ratio [OR] 0.52, 95% confidence interval [CI] 0.31 to 0.86), report arrests or legal supervision (OR 0.63, 95% CI 0.47 to 0.84) or be employed (OR 0.39, 95% CI 0.21 to 0.73) during treatment. In contrast, women were more likely than men to use amphetamines during this time (Figure 1). Patterns of opioid use were similar. Owing to large differences in follow-up periods, a meta-analysis was not possible to look at sex differences in long-term prognosis. Although the quality of evidence was generally low, the researchers concluded that there is a need for improved implementation of sex-specific treatment strategies. CMAJ Open 2015;3:E344–E51.
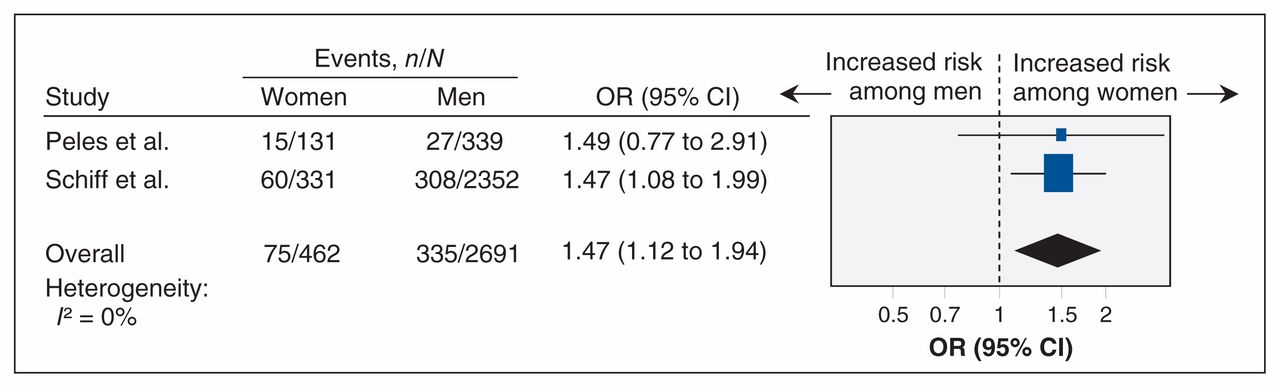
Meta-analysis of sex-related difference in amphetamine use over the past 6 months of treatment among women and men receiving methadone maintenance treatment for opioid use disorders. An odds ratio (OR) greater than 1.0 indicates an increased likelihood of women reporting amphetamine use. CI = confidence interval.
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

