


Abstract
Background: Existing research and media reports convey conflicting impressions of trends in the prevalence of mental illness. We sought to investigate trends in the prevalence of symptoms of mental illness in a large population-based cohort of Canadian children and adolescents.
Methods: We obtained population-based data from the National Longitudinal Survey of Children and Youth. Every 2 years, participants completed self-reported measures of mental illness indicators, including conduct disorder, hyperactivity, indirect aggression, suicidal behaviour, and depression and anxiety. We analyzed trends in mean scores over time using linear regression.
Results: We evaluated 11 725 participants aged 10–11 years from cycles 1 (1994/95) through 6 (2004/05), 10 574 aged 12–13 years from cycles 2 (1996/97) through 7 (2006/07), and 9835 aged 14–15 years from cycles 3 (1998/99) through 8 (2008/09). The distribution of scores on depression and anxiety, conduct and indirect aggression scales remained stable or showed small decreases over time for participants of all ages. The mean hyperactivity score increased over time in participants aged 10–11 years (change per 2-year cycle: 0.16, 95% CI 0.02 to 0.12) and those aged 12–13 years (0.13, 95% CI 0.09 to 0.18). Over time, fewer participants aged 12–13 years (0.40% per cycle, 95% CI −0.78 to −0.07) and aged 14–15 years (0.56% per cycle, 95% CI −0.91 to −0.23) reported attempting suicide in the previous 12 months.
Interpretation: With the exception of hyperactivity, the prevalence of symptoms of mental illness in Canadian children and adolescents has remained relatively stable from 1994/95 to 2008/09. Conflicting reports of escalating rates of mental illness in Canada may be explained by differing methodologies between studies, an increase in treatment-seeking behaviour, or changes in diagnostic criteria or practices.
Popular media tends to perpetuate the idea that the prevalence of mental disorders is increasing. However, research supporting this position has been inconsistent. Several studies have shown increases in recent years,1,2 including among adolescents.3–7 These studies have included parent reports from population samples3,4 and physician diagnoses from electronic medical records.6 In contrast, other studies have reported that the rates of mental illness have decreased or remained stable over time.8–11 To appropriately plan services and policies, a proper understanding of trends in adolescent mental health is crucial. This is particularly relevant in Canada, where policy regarding mental health is currently being reconsidered under such frameworks as the Mental Health Commission of Canada’s 2012 mental health strategy, “Changing Directions, Changing Lives.”12
Many methodologic challenges make it difficult to draw conclusions regarding trends in mental illness. The conflicting reports of changing rates of mental illness in the population may be partially explained by changes in diagnostic criteria, differences in assessment methods or variations in official reporting practices.4 For example, one study found that while diagnosed depression decreased, the incidence of depressive symptoms noted by health professionals increased by threefold from 1996 to 2006.13 These changes may not represent a real change in the rates of depression or depressive symptoms, but rather a change in clinical practice.
Canada’s National Longitudinal Survey of Children and Youth repeatedly included a series of questions from 1994/95 to 2008/09 relevant to many aspects of mental health in children and adolescents, including assessments of conduct disorder, hyperactivity, aggression, depression and anxiety, and suicidal thinking and behaviour. Our primary objective was to investigate trends in the prevalence of symptoms in these areas in 3 specific age groups: 10–11, 12–13 and 14–15 years.
Methods
Study design
This study used data from the National Longitudinal Survey of Children and Youth, which involves a population-based cohort of Canadian children and adolescents followed prospectively every 2 years by Statistics Canada since 1994/95.14 The cohort is considered nationally representative, with the exception of children living on First Nations reserves or Crown lands, in institutions and in some remote regions. This study was designed to collect information about multiple aspects of child health and development. The follow-up rate for the National Longitudinal Survey of Children and Youth from cycle 1 (1994/95) to cycle 8 (2008/2009) was 61%.15 Further details about the cohort, including study design and response rates (mostly above 80% at each wave), are described elsewhere.14,15
The survey included numerous assessments related to child and adolescent mental health. The behaviour scale was adapted from questionnaires used in the Montreal Longitudinal Survey and the Ontario Child Health Study, which were designed to identify children who would most likely qualify for a psychiatric diagnosis based on symptom criteria for the revised 3rd edition of the Diagnostic and Statistical Manual of Mental Disorders.16 This scale has been used in previous studies of child and adolescent adjustment, and has shown good psychometric properties.17,18
In each cycle, participants aged 10 years or older were asked to self-report the frequency of various feelings and behaviours in the past week, with 3 possible responses ranging from “never or not true” to “often or very true.” Each item was assigned a score of 0 to 2 (higher scores indicating a greater degree of mental health problems). Questionnaires were completed on paper, at home in a private setting, and sealed in envelopes to ensure confidentiality.
Composite scores were created by summing item scores on each of 4 subscales relevant to adolescent mental illness: conduct disorder (6 items, e.g., “I kick or hit other people my age”), hyperactivity (7 items, e.g., “I am impulsive, I act without thinking”), indirect aggression (5 items, e.g., “When I am mad at someone, I say bad things behind his/her back”), and symptoms of depression/anxiety (7 items, e.g., “I am not as happy as other people my age” and “I worry a lot”).19 The same items were collected at each cycle, with the exception of 1 hyperactivity item and 1 depression/anxiety item, which were dropped in cycle 4. In the interest of comparability over time, these items were not included in composite scores. All items comprising the final scale are presented in Appendix 1, (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.140064/-/DC1), and frequencies of individual responses to each item are presented in Appendix 2 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.140064/-/DC1). Participants with missing data were excluded. The composite scores showed good internal consistency, as assessed by Cronbach α. The α values ranged from 0.73 (indirect aggression) to 0.79 (depression and anxiety).
Suicidal ideation was assessed by asking the participant, “During the past 12 months, did you seriously consider attempting suicide?” Those who answered yes were additionally asked, “During the past 12 months, how many times did you attempt suicide?”
Covariates
Family socioeconomic status was based on the ratio of family income to corresponding low-income cut-off (i.e., the level below which a family is likely to spend a larger proportion of their income on necessities than the average family), calculated based on family size and area of residence. Rural or urban residence was assessed based on postal code. The sex of the child was reported by parents.
Statistical analysis
Mean scores on conduct, indirect aggression, hyperactivity, and depression and anxiety scales were compared across all cycles. We used linear regression treating time as a continuous variable to test for significant cross-sectional trends in mean scores. In addition, we examined trends in the proportion of individuals reporting suicidal ideation and suicide attempt. To account for the complex survey design, we included normalized sampling weights in the analyses. We used cross-sectional weights to represent the Canadian population at each cycle.
We conducted a sensitivity analysis to test whether the percentage of children with high symptom levels followed a similar pattern over time. For each outcome, a cut-off score was identified based on the top decile at the first available time point for each age group. Trend analysis was conducted to determine whether the percentage of children exceeding these cut-off scores changed over time.
We examined interactions with covariates to test whether linear trends differed for different subgroups of the population (e.g., rural or urban, low income). Interactions with sex were also examined, considering the documented sex differences in prevalence of mental health outcomes, including depression, externalizing behaviours and suicide.20–22 No interactions suggesting an increase in mental illness symptoms for any subgroups were found. Therefore, we present results for all subgroups together within each age-group sample.
Given that sample attrition may result in biased estimates of changes in rates of mental illness symptoms over time,23 we also examined the association between symptoms of mental illness at age 8–9 years and dropout at ages 10–11, 12–13 and 14–15 years.
Results
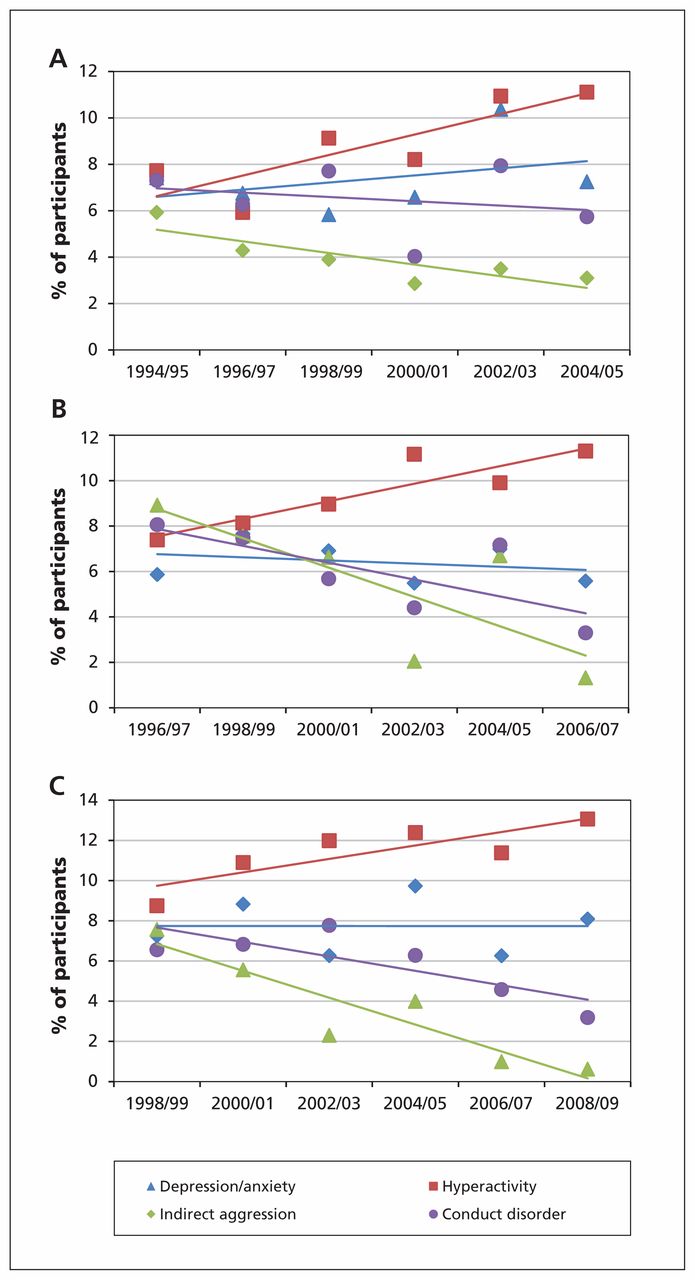
The sample for the present study included 11 725 participants who reported at age 10–11 years (1994/95–2004/05), 10 574 who reported at age 12–13 years (1996/97–2006/07) and 9835 who reported at age 14–15 years (1998/99–2008/09). Participant characteristics are presented in Table 1. Mean scores on the depression and anxiety scale did not change significantly over time among participants aged 10–11 years (0.03 per 2-year cycle, 95% CI −0.01 to 0.07) (Figure 1A; Appendix 3, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.140064/-/DC1) and among participants aged 12–13 years (−0.01, 95% CI −0.05 to 0.03) (Figure 1B, Appendix 3). There was evidence of a small but significant decrease in mean depression and anxiety scores over time for children aged 14–15 years (−0.06, 95% CI −0.10 to −0.01) (Figure 1C, Appendix 3).
Sample characteristics of participants in the National Longitudinal Survey of Children and Youth, by cycle

Mean scores for symptoms of mental illness between 1994/95 and 2004/05 in participants aged 10–11 years (A), between 1996/97 and 2007/08 in those aged 12–13 years (B) and between 1998/99 and 2008/09 in those aged 14–15 years (C). *Higher scores indicate greater symptoms. Possible scores range from 0 to 14 for depression/anxiety and hyperactivity, 0 to 10 for indirect aggression and 0 to 12 for conduct disorder.
Indicators of conduct disorder and indirect aggression decreased slightly but significantly over time in all age groups (Figure 1, Appendix 3). Changes per 2-year cycle in mean scores on the conduct disorder scale decreased among participants aged 10–11 years (−0.04, 95% CI −0.07 to −0.04), 12–13 years (−0.07, 95% CI −0.10 to −0.04) and 14–15 years (−0.06, 95% CI −0.09 to −0.03). Similarly, changes per 2-year cycle in mean scores on the indirect aggression scale decreased among participants aged 10–11 years (−0.11, 95% CI −0.13 to −0.08), 12–13 years (−0.08, 95% CI −0.11 to −0.05) and 14–15 years (−0.04, 95% CI −0.07 to −0.01).
In contrast, there was a significant increase in mean hyperactivity scores (Figure 1, Appendix 3) among participants aged 10–11 years (change per 2-year cycle, 0.16, 95% CI 0.02 to 0.12) and participants aged 12–13 years (0.13, 95% CI 0.09 to 0.18), but not among those aged 14–15 years (0.04, 95% CI −0.01 to 0.09).
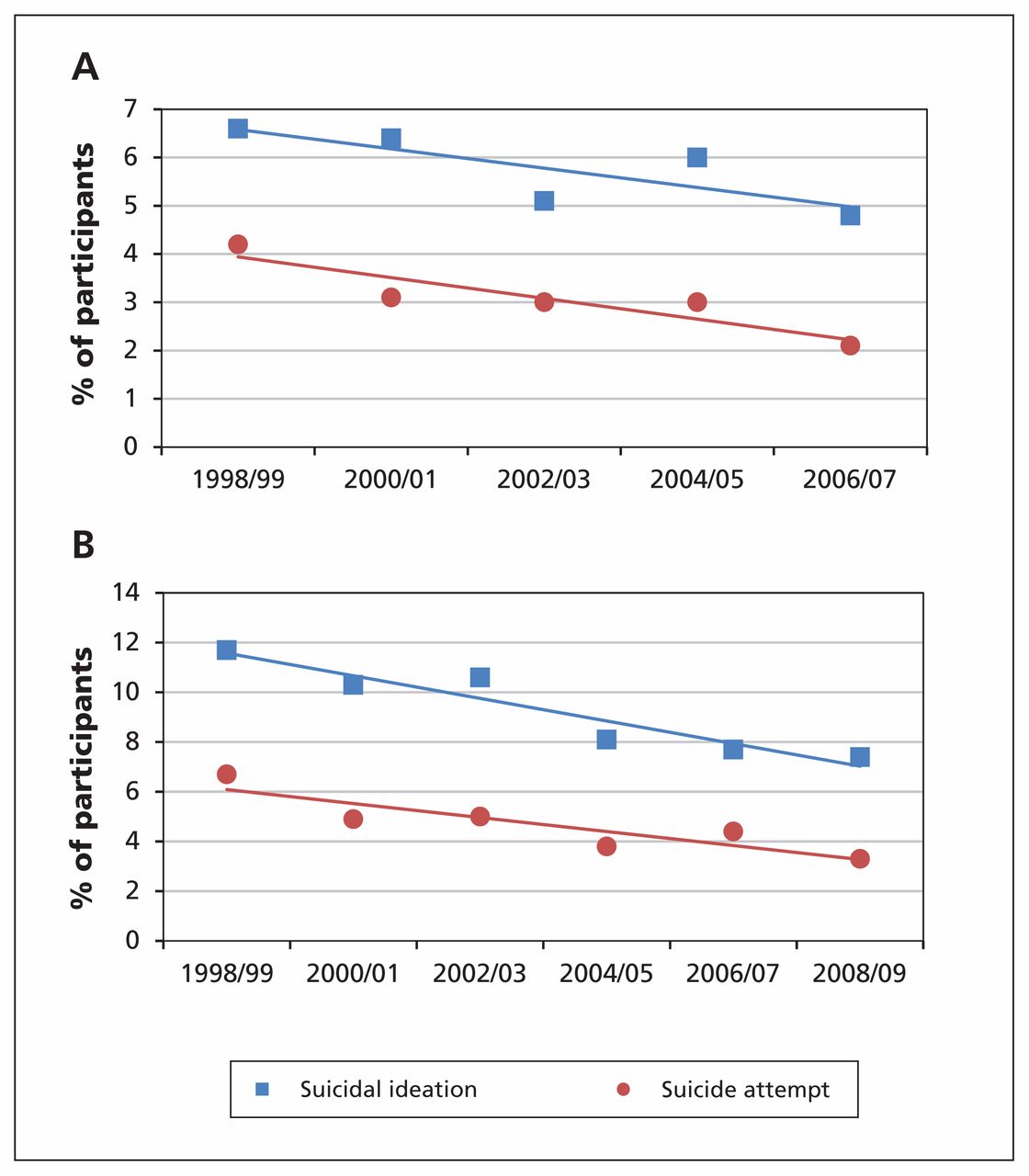
The proportion of participants aged 12–13 and 14–15 years who reported having considered or attempted suicide in the past 12 months declined moderately from 1998/99 to 2008/09 (Figure 2; Appendix 3, supplemental tables 4–5). The percentage of participants aged 12–13 years who had attempted suicide significantly decreased by 0.40% with each 2-year cycle (95% CI −0.78 to −0.07). We also found declining trends in the percentage of adolescents aged 14–15 years who had considered (−0.92%, 95% CI −1.39 to −0.45) and attempted suicide (−0.56%, 95% CI −0.91 to −0.23).

Trends in suicidal ideation and suicide attempt between 1998/99 and 2006/07 in participants aged 12–13 years (A) and between 1998/99 and 2008/09 in those aged 14–15 years (B).
The pattern of results for the sensitivity analysis was nearly identical to that found using mean symptom levels (Figure 3; Appendix 3, supplemental tables 6–8). The only exceptions were among adolescents aged 14–15 years, for whom the percentage reporting high levels of hyperactivity increased significantly over time (change per 2-year cycle, 0.68%, 95% CI 0.15 to 1.22), but the percentage with high depression and anxiety scores did not change significantly over time (0.0%, 95% CI −0.4 to 0.4).
Trends in high scores on mental health indices between 1994/95 and 2004/05 in participants aged 10–11 years (A), between 1996/97 and 2006/07 in those aged 12–13 years (B) and between 1998/99 and 2008/09 in those aged 14–15 years (C). Cut-off scores were calculated based on the top decile at the first available cycle for each age group.
Attrition analysis suggested that the drop-out rate among participants aged 10–15 years was significantly associated with lower symptoms of mental illness at age 8–9 years (data not shown).
Interpretation
Our results suggest that, with the exception of hyperactivity, the prevalence of symptoms of mental health disorders in Canadian children and adolescents is not increasing. In fact, the results suggest that some symptoms of mental illness and behavioural problems seem to be decreasing (i.e., indirect aggression, conduct disorder and suicide attempts). We did find evidence of an increase in hyperactivity among participants aged 10–11 and 12–13 years.
Several studies done in the United States and other countries have reported that the prevalence of mental health disorders in adolescents is increasing.3–7 The current study contrasts with the previous literature by showing relatively stable or declining prevalence between 1994/95 and 2008/09.
There is still a great deal of debate as to the direction of temporal trends in rates of mental illness. Results of meta-analysis support the finding that rates of depression have remained similarly stable among children and adolescents,20 and a recent systematic review reported that most studies suggest similar stability in rates of externalizing problems among children and adolescents.24
Discrepancies in the literature surrounding trends in the prevalence of mental illness in the population may be due in part to differences in measurement. Some studies report results based on disorders diagnosed by a health professional,6,9 and others report results based on face-to-face interviews8,11,25 or reports of symptoms from parents or teachers.3,4 The present study used self-report assessments of symptoms, which may explain why these results differ from some studies. Considerable changes have been made in diagnostic criteria for mental illness, and methods of diagnosing childhood disorders have greatly improved.26 Some studies using a clinical diagnosis of depression have noted increases in rates of mental health problems.6,7 One national Canadian study reported that although self-reported distress symptoms remained stable over time in adults, clinical diagnosis of mood disorders, as well as self-reported antidepressant use, showed an increase.10 However, such results may reflect changes in treatment-seeking behaviour.27
There have been substantial efforts made to reduce the stigma surrounding mental illness,28,29 and awareness of mental illness has increased among medical professionals and the general public.28–30 As mental health literacy increases, parents and caregivers are presumably more likely to recognize mental health problems and refer children to professional care.31,32 This may explain why studies using reports from parents and teachers have reported increases in rates of child and adolescent mental illness,3,4 and why diagnosed rates of mental health problems have increased in recent years.6,7 However, recent research suggests that most youth experiencing mental health problems are still not accessing treatment.28,33,34 Continued effort is needed to reduce barriers to help-seeking behaviour among youth.
Given advances in diagnosis and treatment of mental illness among adolescents, it is possible that observed decreases in symptoms over time may be due to successful treatment. There has been a reported increase in the prescription of stimulants35–37 and antidepressants10,36–40 for children and adolescents in recent years.
In the present study, we found that there was a moderate increase over time in mean hyperactivity score in participants aged 10–11 and 12–13 years. Although these increases were statistically significant, it is unknown whether the magnitude of this change would be considered clinically significant. Previous work has found an upward trend in the prevalence of prescribed medications for attention-deficit/hyperactivity disorder (ADHD) and diagnoses of ADHD in Canadian school-aged children.7,35 A similar upward trend has been reported for US children (aged 3–17 yr) over the same period.41–43 Some authors have hypothesized that increases in ADHD over time may be due to increasing exposure to etiological factors, such as environmental contaminants.43 Other environmental factors, such as the increasing ubiquity of electronic media44 may also contribute to increases in ADHD symptoms over time, though more research is needed to confirm a causal association.
Strengths and limitations
This study has several methodologic strengths. It comprises a large population-based sample broadly representative of the Canadian population. The survey repeatedly included a series of questions relevant to many aspects of mental health. The use of a set of identical instruments and items regarding symptoms of mental illness over a prolonged period provided an excellent opportunity to examine historical trends.
Limitations of this study should be noted. This study used self-reported assessment of symptoms on a continuous scale to measure mental illness rather than a clinical diagnosis. This may be considered an advantage because we were able to include children with moderate or subthreshold symptoms.
The observed stability in rates of mental illness symptoms over time may be due to sample attrition. That is, it is possible that participants with higher scores on symptoms of mental illness may be more likely to drop out of the study over time, which could lead to lower estimates of the rates of mental illness in later collection cycles. However, in the present sample, higher scores on symptoms of mental illness at ages 8–9 years were associated with a lower likelihood of dropping out of the sample at ages 10–15 years, as has been reported in other studies using this cohort.45
The present study reports trends in symptoms of mental illness among youth for the period from 1994/95 to 2008/09. Continued research is necessary to understand how trends may have changed in the time since these data were collected.
Conclusion
Our results suggest that, contrary to popular media reports, symptoms of mental illness (with the exception of hyperactivity) are not increasing among Canadian adolescents. An accurate understanding of trends in adolescent mental health is fundamental to appropriately plan public health services and policy. There has been an increase in suicide prevention efforts since the mid-1990s.46,47 Encouragingly, results from this study suggest that suicidal ideation and suicide attempts may be declining. This finding is supported by studies that reported a recent decline in suicide rates48–50 and attempts51 among Canadian and American youth. Though there is no conclusive evidence for the efficacy of various efforts in preventing suicide,52 some strategies, including physician education and certain school-based strategies, show promise in reducing suicidal behaviours.46,47,50,53 Continued effort in suicide prevention, rigorous research into the efficacy of prevention programs, and improved interventions targeting mental illness in adolescents is crucial for improving the mental health of Canadian adolescents.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
-
Contributors: Ian Colman conceived and designed the study. Seanna McMartin and Mila Kingsbury performed the data analysis and wrote the manuscript. All of the authors contributed to the study design, interpreted the results, revised the manuscript, approved the final version submitted for publication and agree to act as guarantors of the work.
-
Funding: This research was supported by a grant from the SickKids Foundation and the Canadian Institutes of Health Research (grant no. SKF 116328), as well as funding from the Canada Research Chairs program for Ian Colman. The funders had no role in the design or conduct of the study; the collection, management, analysis or interpretation of the data; the preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication. The research and analysis are based on data from Statistics Canada; the opinions expressed do not represent the views of Statistics Canada.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Suicidality among sexual minority and transgender adolescents: a nationally representative population-based study of youth in Canada
- Physical-mental multimorbidity in children and youth: a scoping review
- Effect of serotonin modulating pharmacotherapies on body mass index and dysglycaemia among children and adolescents: a systematic review and network meta-analysis protocol
More in this TOC Section
Similar Articles
Collections

