


Abstract
Background: It is unclear whether a healthy lifestyle mitigates the adverse effects of job strain on coronary artery disease. We examined the associations of job strain and lifestyle risk factors with the risk of coronary artery disease.
Methods: We pooled individual-level data from 7 cohort studies comprising 102 128 men and women who were free of existing coronary artery disease at baseline (1985–2000). Questionnaires were used to measure job strain (yes v. no) and 4 lifestyle risk factors: current smoking, physical inactivity, heavy drinking and obesity. We grouped participants into 3 lifestyle categories: healthy (no lifestyle risk factors), moderately unhealthy (1 risk factor) and unhealthy (2–4 risk factors). The primary outcome was incident coronary artery disease (defined as first nonfatal myocardial infarction or cardiac-related death).
Results: There were 1086 incident events in 743 948 person-years at risk during a mean follow-up of 7.3 years. The risk of coronary artery disease among people who had an unhealthy lifestyle compared with those who had a healthy lifestyle (hazard ratio [HR] 2.55, 95% confidence interval [CI] 2.18–2.98; population attributable risk 26.4%) was higher than the risk among participants who had job strain compared with those who had no job strain (HR 1.25, 95% CI 1.06–1.47; population attributable risk 3.8%). The 10-year incidence of coronary artery disease among participants with job strain and a healthy lifestyle (14.7 per 1000) was 53% lower than the incidence among those with job strain and an unhealthy lifestyle (31.2 per 1000).
Interpretation: The risk of coronary artery disease was highest among participants who reported job strain and an unhealthy lifestyle; those with job strain and a healthy lifestyle had half the rate of disease. A healthy lifestyle may substantially reduce disease risk among people with job strain.
Psychosocial work stress, denoted by job strain, is associated with an elevated risk of coronary artery disease.1–7 This association is apparent across strata of sex, age, socioeconomic status and region, and it does not appear to be completely explained by confounding.7 For many people, avoidance of stress at work is unrealistic. The absence of strong evidence for effective interventions to reduce job strain therefore raises the challenge of identifying additional approaches for dealing with the health impact of stress in the workplace.
Guidelines for the prevention of heart disease emphasize the importance of a healthy lifestyle — physical activity, a healthy diet (and healthy weight) and not smoking — in lowering disease risk.8–11 Whether a healthy lifestyle offsets the deleterious impact of job strain on coronary artery disease remains unclear. A straightforward approach to test this hypothesis would involve comparing the rates of coronary artery disease among people with job strain and an unhealthy lifestyle with the rates among those with job strain and a healthy lifestyle. If a marked difference is apparent, one would consider a healthy lifestyle to be the likely factor contributing to the reduced risk among those with job strain. However, such stratifications require a large, well-characterized dataset, which to date has been lacking. We pooled individual-level data for more than 100 000 men and women participating in 7 cohort studies to examine the combined associations of job strain and lifestyle with risk of coronary artery disease.
Methods
Study population
We used pooled individual-level data from 7 European prospective cohort studies participating in the Individual-participant-data Meta-analysis in Working Populations (IPD-Work) Consortium:7 the Whitehall II Study in the United Kingdom;12 the GAZEL Study in France;13 the Belgian Job Stress Project (Belstress);14 the Work, Lipids, and Fibrinogen Study in Stockholm (WOLF-S)15 and in Norrland (WOLF-N),16 Sweden; the Finnish Public Sector Study;17 and the Health and Social Support (HeSSup) Study in Finland.18 Details of the study design and participants have been published previously and are summarized in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121735/-/DC1).12–18
For our meta-analysis, we included all men and women from the cohort studies who were free of coronary artery disease at baseline (1985–2000 depending on the year recruitment began) and for whom complete data on job strain, lifestyle risk factors and coronary artery disease were available. Mean follow-up for incident coronary artery disease ranged from 3.1 to 15.1 years depending on the study.
Ethics approval
Each constituent study in the IPD-Work Consortium was approved by the relevant local or national ethics committees, and all participants gave informed consent to take part.
Measurement of job strain and lifestyle risk factors
Predefined, harmonized measures were used to assess job strain (yes v. no) and 4 lifestyle risk factors at baseline: current smoking (yes v. no),19 physical inactivity (yes v. no),20 heavy drinking (≥ 21 and ≥ 28 units of alcohol per wk for women and men, respectively),21 and obesity (body mass index [BMI] ≥ 30).22 A detailed description of these measures, including their validation and harmonization, has been published previously.19,23,24 In brief, questions used to measure job strain were taken from a validated job-content questionnaire and demand–control questionnaire and were included in all studies at baseline (sample statement/question: “My job requires working very hard,” “Do you have the possibility of learning new things through your work?”).23 All items required responses on a Likert-type scale (e.g., 1 = “never or very seldom” and 5 = “almost always or very often”).
We calculated job-demand and job-control scales using the mean response scores for individual questions. Job strain was defined as having a job with high demands (a job-demand mean score above the study-specific median) and low control (a job-control mean score below the study-specific median); “no job strain” was denoted by all other combinations of demands and control.23 In a previous report from the IPD-Work Consortium, the collective measure of job strain rather than its components (demands and job control separately) was found to be associated with risk of coronary artery disease.7
Tobacco smoking, alcohol intake and physical inactivity were ascertained from participant-completed questionnaires in all of the studies.19–21 Enquiries were made about the total number of alcoholic drinks, by type of drink, consumed in a week.21 “One drink” was defined as the equivalent of about 1 unit or 1 glass of alcoholic drink or 10 g of ethanol. Men who consumed 28 or more drinks per week and women who had 21 or more drinks per week were classified as heavy drinkers.25 Physical inactivity was defined as no or very little moderate or vigorous leisure-time physical activity or exercise.20 The data on physical activity varied across studies, with examples of definitions of physical inactivity such as “no weekly leisure-time physical activity” and “no or very little exercise, or only occasional walks.” 20 We calculated BMI using data for height and weight, which were self-reported in 3 studies13,17,18 and measured directly in 4 studies.12,14–16 Obesity was defined as a BMI of 30 or greater.22
We grouped the participants into 3 lifestyle categories: healthy lifestyle (no lifestyle risk factors), moderately unhealthy lifestyle (1 risk factor) and unhealthy lifestyle (2–4 lifestyle risk factors).
Outcome measure
The primary outcome was incident coronary artery disease, defined as first nonfatal myocardial infarction or cardiac-related death. Participants were followed from baseline to the earliest occurrence of incident coronary artery disease, death or the end of the registry follow-up.7 Nonfatal myocardial infarction was identified according to the criteria from the World Health Organization MONICA (Multinational Monitoring of Trends and Determinants in Cardiovascular Disease) Project,26 the International Classification of Diseases, 9th Revision (ICD-9) code 410, or ICD-10 codes I21–I22. Deaths were classified as cardiac related if either ICD-9 codes 410–414 or ICD-10 codes I20–I25 were cited on the death certificate.
Statistical analysis
We pooled the data from the participating cohort studies after harmonization of all measures. To examine the absolute difference in risk between groups, we computed age-, sex- and cohort-adjusted 10-year incidence of coronary artery disease by baseline measures of job strain, lifestyle risk factors and combinations of both. Hazard ratios (HRs) and 95% confidence intervals (CIs) were computed using Cox regression. To examine whether the associations of the combinations of job strain and lifestyle risk factors with the risk of coronary artery disease were confounded by social patterning of these characteristics, we adjusted the models for socioeconomic status. To account for differences between countries in which the cohort studies were conducted, the models were adjusted for country. We also entered job strain and lifestyle category in a model simultaneously to ascertain whether they were independently associated with risk of coronary artery disease. All analyses were performed with the use of SAS 9.2 statistical software (SAS Institute Inc., Cary, North Carolina).
We calculated population attributable risk for 3 exposures: job strain, unhealthy lifestyle and their combination, as described in Appendix 2 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121735/-/DC1). Population attributable risk is the estimated proportion of all cases of coronary artery disease that are attributable to the exposure; it assumes a causal association between risk factor and disease.
Results
A total of 102 128 men and women from the cohort studies met the inclusion criteria. The baseline characteristics of the pooled study population are shown in Table 1. The mean age was 44.3 (range 17–70) years; 51.8% of the participants were women. Overall, 15 986 (15.7%) of the participants reported job strain. Cohort-specific figures are provided in Appendix 3 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121735/-/DC1).
Characteristics of 102 128 men and women free of coronary artery disease at baseline in 7 cohort studies
A total of 1086 participants had incident events of coronary artery disease during 743 948 person-years at risk (mean follow-up 7.3 years). The crude 10-year incidence of coronary artery disease was 14.6 per 1000 people. The 10-year rates by job strain and lifestyle risk factors, adjusted for age, sex and cohort, are shown in Table 2. The rate was 18.4 per 1000 among participants with job strain and 14.7 per 1000 among those without job strain, for a difference of 3.7 events per 1000. The corresponding HR was 1.25 (95% CI 1.06–1.47) and population attributable risk 3.8%. The 10-year incidence was 30.6 per 1000 among participants with an unhealthy lifestyle, 17.8 per 1000 among those with a moderately unhealthy lifestyle and 12.0 per 1000 among those with a healthy lifestyle. Participants with an unhealthy lifestyle had 18.6 more events per 1000 than those with a healthy lifestyle (HR 2.55, 95% CI 2.18–2.98). The population attributable risk for unhealthy and moderately unhealthy lifestyles versus a healthy lifestyle was 26.4%. Relative to the group in which the risk factor was absent, age-, sex- and cohort-adjusted HRs for single lifestyle risk factors were 2.14 (95% CI 1.89–2.44) for current smoking, 1.19 (95% CI 0.98–1.44) for heavy drinking, 1.52 (95% CI 1.32–1.74) for physical inactivity and 1.67 (95%CI 1.41–1.98) for obesity.
Age-, sex- and cohort-adjusted 10-year incidence of coronary artery disease by job strain, lifestyle risk factors and their combinations at baseline
The risk of coronary artery disease associated with combinations of job strain and individual lifestyle risk factors, adjusted for age, sex and cohort, is shown in Figure 1. Having any of the lifestyle risk factors of smoking, physical inactivity or obesity but no job strain was associated with an increased risk of coronary artery disease. The addition of job strain to obesity increased the risk of coronary artery disease, but the risk did not increase appreciably when job strain was added to smoking, heavy drinking or physical inactivity.
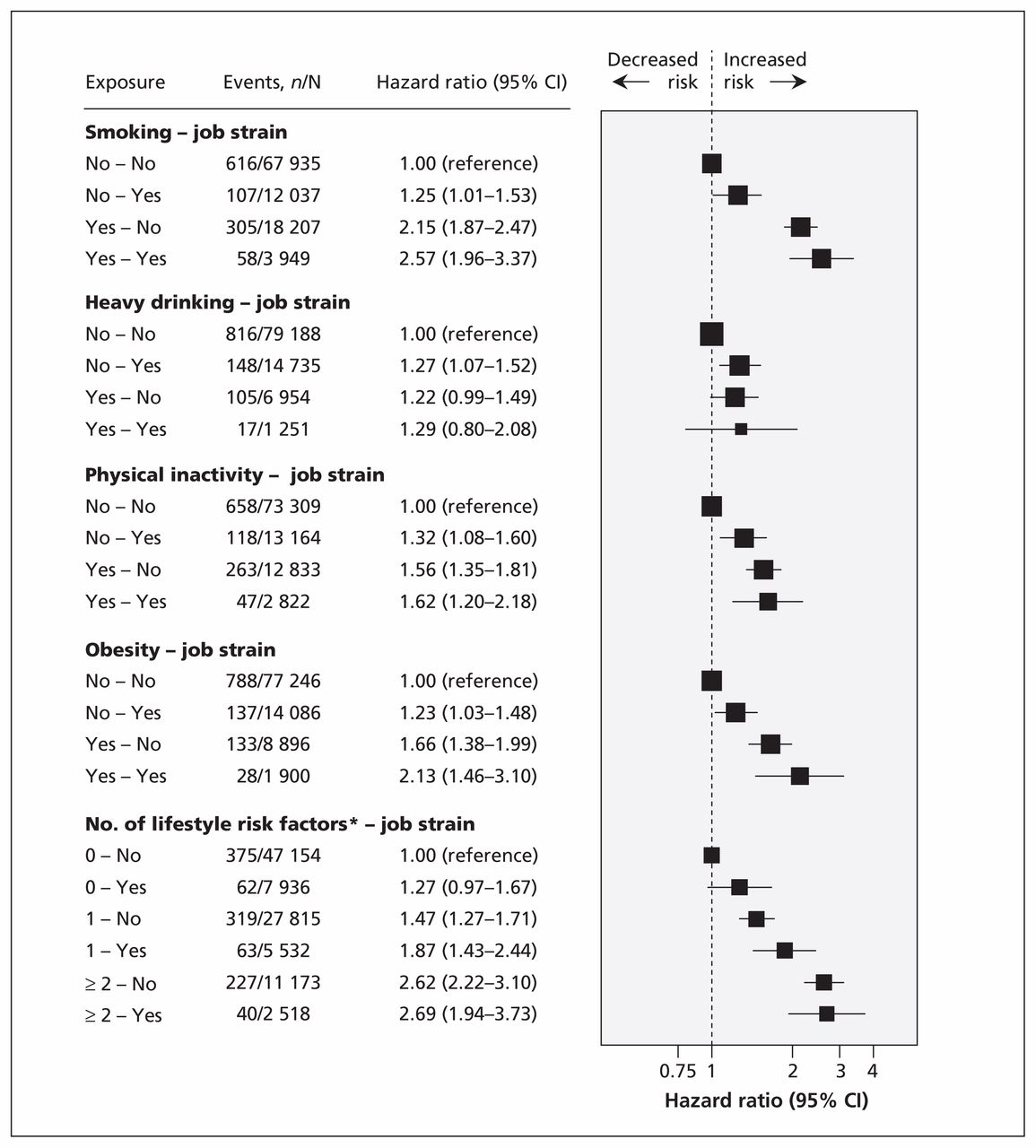
Associations of lifestyle risk factors and job strain with risk of coronary artery disease after adjustment for age, sex and cohort. Values greater than 1.0 indicate an increased risk of incident coronary artery disease. CI = confidence interval. *0 risk factors = healthy lifestyle, 1 risk factor = moderately unhealthy lifestyle and ≥ 2 risk factors = unhealthy lifestyle.
Our analyses of the combinations of job strain and lifestyle categories (unhealthy, moderately unhealthy and healthy) associated with risk of coronary artery disease are also shown in Figure 1. The adjusted HR for a combination of job strain and an unhealthy lifestyle compared with no job strain and a healthy lifestyle was 2.69 (95% CI 1.94–3.73). Among participants who reported job strain, the 10-year incidence of coronary artery disease was 31.2 per 1000 people for those with an unhealthy lifestyle and 14.7 per 1000 for those with a healthy lifestyle, for a difference of 16.5 events per 1000 (Table 2). Among participants with a healthy lifestyle but no job strain, the corresponding incidence was 11.6 per 1000 (3.1 events lower than the rate among those with a healthy lifestyle and job strain).
In multivariable analyses, job strain and lifestyle were independently associated with risk of coronary artery disease. In a multivariable model including age, sex and cohort, mutual adjustment for job strain and lifestyle yielded a HR of 1.21 (95% CI 1.03–1.43) for job strain relative to no job strain, and 1.77 (95% CI 1.57–2.00) for an unhealthy versus healthy lifestyle. There was no evidence of an interaction between job strain and lifestyle on coronary artery disease (p = 0.6).
Results from the analyses in which we adjusted for socioeconomic status in addition to age, sex and cohort are shown in Appendix 4 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121735/-/DC1). This additional adjustment had little effect on estimates shown in Figure 1. For example, the adjusted HR for a combination of job strain and an unhealthy lifestyle compared with no job strain and a healthy lifestyle was 2.47 (95% CI 1.77–3.44). In a model adjusted for age, sex and country, the corresponding HR was 2.50 (95% CI 1.80–3.46). There was no evidence of an interaction between sex and job strain–lifestyle combinations (p = 0.5), between country and job strain–lifestyle combinations (p = 0.2) or between cohort and job strain–lifestyle combinations (p = 0.9).
Interpretation
In our meta-analysis of individual-level data for more than 100 000 participants in 7 prospective cohort studies, we found that the risk of coronary artery disease was highest among those who reported job strain and an unhealthy lifestyle at baseline. Participants who reported job strain but who had a healthy lifestyle had about half the rate of disease. These findings suggest that a healthy lifestyle is associated with a reduced risk of coronary artery disease among people with job strain. Our findings were robust to adjustment for socioeconomic status, and there was no evidence of heterogeneity of effects according to sex, cohort or country.
We assume that the difference in the 10-year incidence of coronary artery disease between the participants with a healthy lifestyle and those with an unhealthy lifestyle was due to the favourable effects of healthy behaviours. This assumption is justified because evidence from randomized controlled trials have shown that lifestyle changes can reduce disease risk. In trials of weight reduction interventions, for example, weight loss resulted in reduced blood pressure and hypertension27,28 and improved high-density lipoprotein cholesterol levels among overweight and obese individuals.29 In a trial with an extended 15-year follow-up, an intensive smoking cessation program followed by 5 years of reinforcement reduced mortality among individuals with airway obstruction.30 Other randomized controlled trials have been based on short-term interventions (e.g., smoking advice) or have targeted patients with prevalent cardiovascular disease.31,32 Evidence for the beneficial effects of physical activity33,34 and the adverse effects of high alcohol consumption25,35,36 and job strain7,37 on heart disease is mostly limited to observational studies. Nevertheless, the findings obtained are robust and demonstrate dose–response associations even after adjustment for other relevant risk factors.
Numerous studies have examined the associations of lifestyle-related factors27–30,33–36,38 and work stress6 with coronary artery disease, but few have had sufficient power to examine their combined effects. One exception is the INTERHEART case–control study, which recruited about 11 000 patients with incident myocardial infarction and more than 11 000 controls from 52 countries.2,38 The investigators found that work stress was associated with a doubling of the odds of myocardial infarction38 — a stronger association than in our study (1.25-fold excess risk of incident coronary artery disease). Because the INTERHEART study assessed risk factors after disease ascertainment, the disease event may have affected perceptions of stress levels, thus leading to reverse causality. This is a less likely explanation for our findings, which are based on a prospective study design.
Strengths and limitations
Our study has some notable strengths. We extracted data from studies in 2 stages: the exposure was defined and harmonized across cohorts, with investigators masked to the health outcome; outcome data were obtained after this stage to minimize investigator bias.24 We calculated population attributable risk and absolute differences in incidence rates between groups, in addition to HRs, because absolute differences in disease risk are considered to be particularly useful for planning public health policy.
Our results also have limitations. Job strain, as well as smoking status, alcohol intake and physical activity, were self-reported by participants; therefore, some misclassification of these lifestyle indicators may have occurred. Our study was based on observational data; thus, conclusions about causal associations with coronary artery disease are precluded because we cannot rule out residual or unmeasured confounding. However, because no large-scale randomized controlled trials have examined job strain and lifestyle risk factors in relation to heart disease incidence, observational studies provide the best available evidence for clinical practice.
Conclusion
In our meta-analysis of pooled data from prospective cohort studies, the risk of coronary artery disease was highest among participants who reported job strain and an unhealthy lifestyle; those with job strain and a healthy lifestyle had about half the rate of this disease. These observational data suggest that a healthy lifestyle could substantially reduce the risk of coronary artery disease among people with job strain. In addition to stress counselling, clinicians might consider paying closer attention to lifestyle risk factors in patients who report job strain.
Acknowledgements
Mika Kivimäki is supported by a grant from the Medical Research Council (grant no. K013351) and a professorial fellowship from the Economic and Social Research Council. Andrew Steptoe is a British Heart Foundation Professor. David Batty was a Wellcome Trust Fellow during the preparation of the original manuscript.
Footnotes
Competing interests: Töres Theorell receives royalties for books written on various topics, including psychosocial factors; music and health; and Sweden’s working life in the 1990s. Hugo Westerlund’s institution has received a research grant from Saint-Gobain Ecophon AB, a manufacturer of sound-absorbing materials, to study the effect of such materials on stress, job satisfaction and productivity in open-plan offices. No competing interests declared by the other authors.
This article has been peer reviewed.
Contributors: Mika Kivimäki and David Batty drafted the manuscript, and Solja Nyberg performed the statistical analyses. All of the authors contributed to the design of the study, interpreted the results, revised the manuscript and approved the final version submitted for publication.
Funding: The IPD-Work Consortium is supported by the EU New OSH ERA Research Programme (funded by the Finnish Work Environment Fund, the Swedish Council for Working Life and Social Research, the German Social Accident Insurance and the Danish National Research Centre for the Working Environment), the Academy of Finland (grant no. 132944), the Bupa Foundation in the UK, and the Ministry of Social Affairs and Employment in the Netherlands. The German National Accident Insurance supports analyses in the frame of the OSH ERA project. Funding bodies for participating cohort studies are listed on their websites. The study sponsors had no role in the design of the study, the collection, analysis or interpretation of data, the writing of the report or the decision to submit the article for publication.
References
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Increased all-cause mortality following occupational injury: a comparison of two states
- Multicohort study of change in job strain, poor mental health and incident cardiometabolic disease
- Longitudinal study of occupational noise exposure and joint effects with job strain and risk for coronary heart disease and stroke in Swedish men
- Job strain and the incidence of coronary heart diseases: does the association differ among occupational classes? A contribution from a pooled analysis of Northern Italian cohorts
- Prevalence of cardiovascular health and its relationship with job strain: a cross-sectional study in Taiwanese medical employees
- Association between job strain and risk of incident stroke: A meta-analysis
- The association between job strain and atrial fibrillation in Swedish men
- Job Strain as a Risk Factor for Type 2 Diabetes: A Pooled Analysis of 124,808 Men and Women
- A longitudinal general population-based study of job strain and risk for coronary heart disease and stroke in Swedish men
- Job strain and lifestyle factors
- Job strain, health behaviours and heart disease
More in this TOC Section
Similar Articles

