


Gallstone disease is responsible for about 1.8 million ambulatory care visits and more than 700 000 cholecystectomies yearly in the United States.1,2 In Canada, the adjusted annual rate of elective cholecystectomy was 260.8 per 100 000 population during the period 1992–2000.3 Gallstone disease is the second most common reason for hospital admissions (with an estimated cost of US$5.8 billion annually), although only 15% of people with gallstones have related symptoms.4–7 One complication is the occurrence of stones in the common bile duct.4–7
Stones in the common bile duct most commonly result from the passage of gallstones through the cystic duct into the common bile duct. Less frequently, they may originate in the common bile duct itself. Stones in the common bile duct can cause biliary obstruction, cholangitis, pancreatitis, or secondary biliary cirrhosis in patients who have had the stones for a long time. More than 1 in 10 patients (10%–18%) undergoing cholecystectomy for gallstones have concomitant common bile duct stones,7 and up to 3.8% have symptoms related to common bile duct stones during the first year after cholecystectomy.8
The management of patients with gallstone disease suspected of having stones in the common bile duct has three aims: to evaluate the probability of stones in the common bile duct, to treat these stones when present, and to treat the stones in the gallbladder. In this article, we review the development of practical approaches to the first two aims. A summary of the evidence we used in our review is available in Box 1. Most of the identified studies describing the natural history of common bile duct stones and relevant imaging modalities were observational in design; studies reporting therapeutic outcomes were based on randomized trials and meta-analyses.
Summary of the literature review
We performed a literature search of the Embase (1980 to October 2011), MEDLINE (1950 to October 2011) and Cochrane Library databases. We used a combination of MeSH subject headings and text words, including “choledocholithiasis,” “cholelithiasis,” “common bile duct stone,” “intraoperative cholangiography,” “operative cholangiography,” “perioperative cholangiogram,” “rendezvous,”and “meta-analysis.” Reference lists from selected articles were reviewed manually to identify additional articles. All data were abstracted and recorded in dedicated forms and reviewed by two of us (M.A.A., A.N.B.). Resolution of any discrepancies in data abstraction was achieved through consensus involving a third person (J.S.B.). We included trials with the highest level of evidence; observational studies were included if no controlled trials were available. (For details of the search strategy, see Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110896/-/DC1).
When should common bile duct stones be suspected?
Symptoms and signs suggestive of common bile duct stones can occur in people with intact gallbladders as well as those who have had a cholecystectomy. The clinical presentation includes abdominal pain, jaundice, nausea, vomiting, fever, cholangitis, pancreatitis, and elevated levels of bilirubin or liver enzymes. Patients may also require investigation following an incidental finding of a dilated common bile duct or a stone in the common bile duct, or both.
Because direct cholangiography is often invasive, involving the injection of a contrast agent directly into the common bile duct, many predictive clinical models for common bile duct stones have been proposed (Table 1).9–15 A meta-analysis showed that the best predictors of common bile duct stones in patients before cholecystectomy were cholangitis (likelihood ratio 18.3, 95% confidence interval [CI] 9.0–37.1), and preoperative jaundice and ultrasound evidence of stones in the common bile duct (likelihood ratio > 10 in each case).5 A dilated common bile duct on ultrasound, hyperbilirubinemia and jaundice had likelihood ratios between 4 and 7. More modest predictors included an elevated alkaline phosphatase level, pancreatitis, cholecystitis and hyperamylasemia.
Predictive models for stratifying patients suspected of having stones in the common bile duct
The pattern of fluctuation of liver enzyme levels over time has also been shown to be predictive. In a prospective study involving 94 consecutive symptomatic patients, only 13% of patients whose liver enzyme levels returned to normal rapidly (within 4.8 [standard deviation (SD) 1.6] days) were found to have common bile duct stones by means of cholangiography, as compared with 94% of patients whose levels were increasing (p < 0.001).16
The evaluation of common bile duct stones in patients with gallstone disease involves stratifying their probability of having a stone in the common bile duct to: low (< 10%), intermediate (10%–50%) or high (> 50%)17 (Table 1).
Which imaging modalities are useful?
Many imaging modalities are available for investigating suspected stones in the common bile duct (Table 2). These include older techniques such as intravenous cholangiography and endoscopic retrograde cholangiopancreatography (ERCP) and newer techniques such as magnetic resonance cholangiopancreatography and endoscopic ultrasonography (examples of images obtained with some of these modalities appear in Appendix 3, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110896/-/DC1). A systematic review compared these approaches; however, the included studies were heterogeneous, varying in quality and choice of “gold standard.”4 In most instances, preoperative diagnosis of stones in the common bile duct involves a context-sensitive approach based on the pre-procedural probability of the stones as discussed earlier (Table 1), rather than the routine use of any of these modalities. Variations exist in the availability and expertise of these techniques.
Imaging modalities for detecting stones in the common bile duct4
What is the optimal approach to management?
The optimal strategy is based on clinical information and the patient’s likelihood of having a stone in the common bile duct. For example, in a retrospective study including 1097 consecutive patients who underwent laparoscopic cholecystectomy, Tham and colleagues found that limiting preoperative ERCP to patients with an elevated bilirubin level (> 34 μmol/L) or evidence of stones on ultrasonography or computed tomography (CT) would have decreased the number of unnecessary ERCPs by 50%.18
Stratification of the probability of common bile duct stones was used in a prospective study involving 440 patients undergoing laparoscopic cholecystectomy. It was used to select the approach to imaging and management: ERCP if the probability is extremely high, magnetic resonance cholangiopancreatography if it is high, laparoscopic cholecystectomy with intraoperative cholangiography if it is intermediate, and laparoscopic cholecystectomy without intraoperative cholangiography if the probability is low.6 The use of this stratification system resulted in the discriminatory detection of stones in 92.6%, 32.4%, 3.8% and 0.9% of the patients respectively.6 The proportion of patients with retained stones after two years was 1.4%.
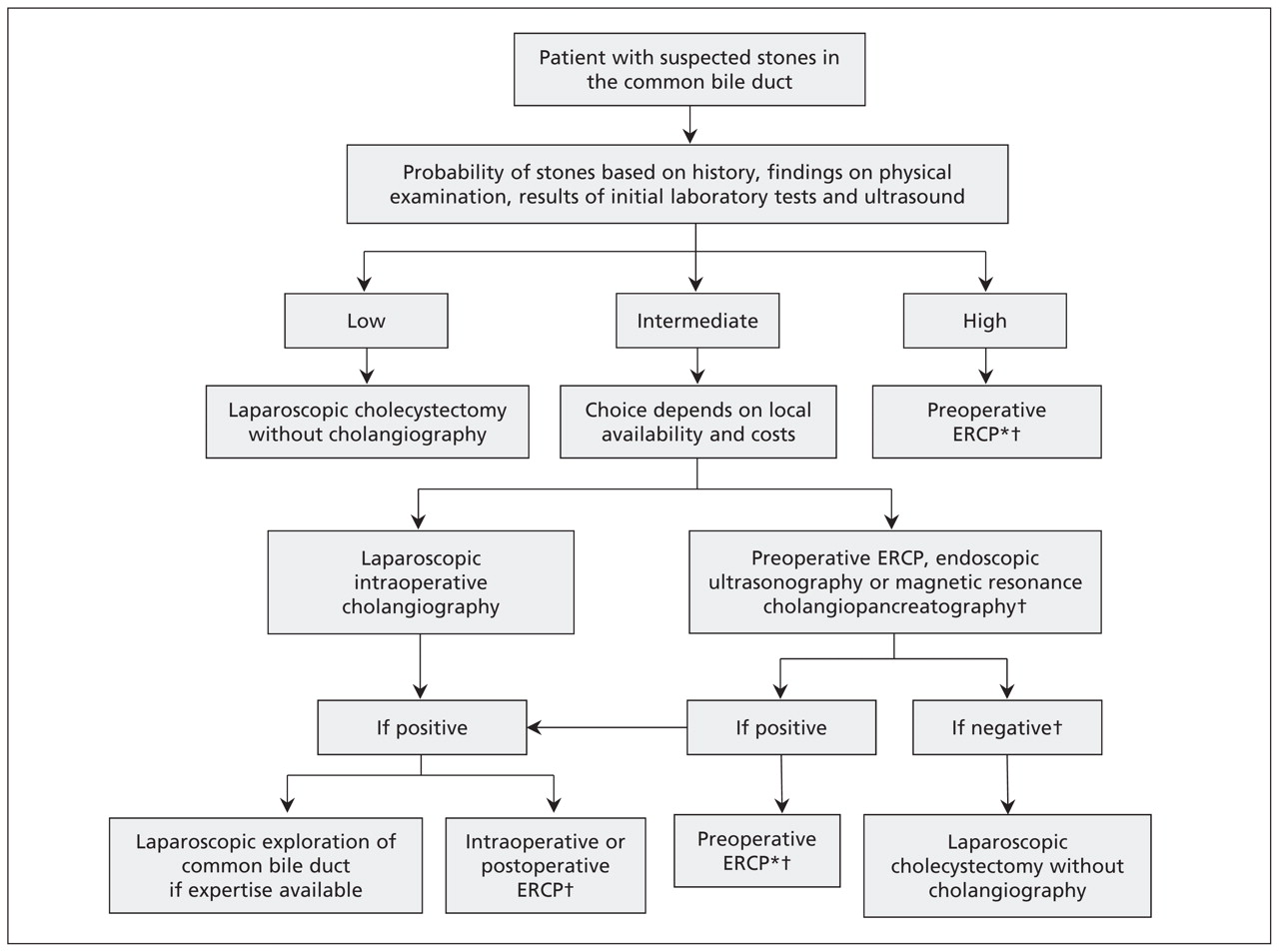
On the basis of findings in the current literature, we propose a simplified algorithm for the management of patients with suspected common bile duct stones before laparoscopic cholecystectomy (Figure 1). The algorithm is similar to one issued by the American Society for Gastrointestinal Endoscopy.17 Several organizations have published guidelines on selected aspects of the management of common bile duct stones (Table 3;1,17,19–27 see also Appendix 4, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110896/-/DC1).

Elective management of suspected stones in the common bile duct before laparoscopic cholecystectomy. *If endoscopic retrograde cholangiopancreatography (ERCP) fails, open cholecystectomy with exploration of common bile duct should be considered. †When the result of imaging test is negative, no further cholangiography is required unless clinical suspicion persists.
Selected statements from guidelines on the management of patients with or suspected of having common bile duct stones
What treatment options are available?
Once popular, open surgical techniques have been superseded by endoscopic techniques. The most common treatment modality is ERCP, with duct cannulation and clearance rates reaching 98% in expert hands.28 Intraoperative ERCP at the time of laparoscopic cholecystectomy (also called “laparoendoscopic rendezvous”) is practised in some centres. It may have advantages, but it presents substantial logistical challenges. It involves the placement of a wire through the cystic duct to the ampulla at the time of laparoscopic cholecystectomy to ensure successful ERCP cannulation.
Open surgical exploration of the common bile duct was historically combined with intraoperative cholangiography at open cholecystectomy to diagnose and treat common bile duct stones. In the era of laparoscopic cholecystectomy, surgical options have been limited mainly to intraoperative cholangiography and occasional transcystic stone removal. The surgical removal of common bile duct stones, whether open or laparoscopic, has become a seldom-performed operation, usually reserved for patients in whom ERCP has failed. Laparoscopic exploration of the common bile duct may be considered in patients with larger stones, but it is practised by few groups.
A Cochrane meta-analysis7 reviewed 13 randomized controlled trials with 12 predefined outcomes in a variety of clinical scenarios. The findings are summarized below, modified to include the option of intraoperative ERCP.
ERCP versus open surgery
In the era of open cholecystectomy, open exploration of the common bile duct was found to be superior to ERCP in achieving stone clearance (odds ratio [OR] 2.89, 95% CI 1.81–4.61).7 Open exploration remains a safe approach and is the “gold standard” if ERCP fails. Hepaticojejunostomy is reserved for the rare patient with many stones.
Pre-or postoperative ERCP versus laparoscopic cholecystectomy
Laparoscopic clearance of stones from the common bile duct was found to be as effective as preoperative (OR 1.00, 95% CI 0.53–1.80) and postoperative ERCP (OR 2.27, 95% CI 0.37–13.9), with no significant difference in morbidity and mortality between the study groups.7 Conversion rates from laparoscopic to open cholecystectomy ranged from 1.3% to 7.4%.7,29 An increased number of total procedures per patient was seen among those undergoing ERCP, whereas shorter hospital stays were seen among those undergoing laparoscopic cholecystectomy.7
Pre-versus intraoperative ERCP
Randomized trials showed that intraoperative ERCP at the time of laparoscopic cholecystectomy (laparoendoscopic rendezvous) was less costly than preoperative ERCP and resulted in decreased morbidity.30–32 This decreased morbidity may especially be true for patients at high risk of ERCP-induced pancreatitis,16 such as those with previous post-ERCP pancreatitis, those with suspected dysfunction of the sphincter of Oddi and those with a normal bilirubin level.33 In one trial, 123 patients at intermediate risk of common bile duct stones were randomly assigned to undergo either preoperative ERCP followed by laparoscopic cholecystectomy, or laparoendoscopic rendezvous. The rates of total morbidity (23% v. 8.5%, p = 0.03), post-ERCP morbidity (18.8% v. 5.1%, p = 0.02) and post-ERCP pancreatitis (12.7% v. 1.7%, p = 0.03) were greater in the group that underwent preoperative ERCP. The length of hospital stay (8 [SD 5] days v. 5 [SD 3] days, p < 0.001) and costs were lower in the intraoperative ERCP group, but the operative times were longer.30 Similar results were obtained in a randomized trial involving patients whose stones were diagnosed by means of magnetic resonance cholangiopancreatography.31 Intraoperative ERCP at the time of laparoscopic cholecystectomy, although less costly, may be logistically challenging and prolongs operative times.
If a patient has had a cholecystectomy in the past and stones are suspected in the common bile duct, a nonoperative approach is usually recommended to avoid repeat surgery,7 although we found no data from randomized trials to support this view.
What is the best way to deal with large stones?
Failure rates with conventional ERCP for the removal of large stones in the common bile duct can reach 20%,7 requiring supplementary specialized techniques (Appendix 5, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110896/-/DC1).
Endoscopic papillary balloon dilation of the ampullary orifice was proposed for the removal of common bile duct stones and the possible prevention of theoretical and largely unproven long-term complications related to the destruction of the sphincter mechanism. This specialized technique has been shown to have lower rates of bleeding and infection compared with conventional sphincterotomy,34,35 but it is not practised in North America because of the elevated risk of pancreatitis noted in a sentinel North American trial.36 This high complication rate37 has not been duplicated in Asian trials.38 More recently, endoscopic papillary balloon dilatation following a small sphincterotomy has been reported39 and is rapidly becoming the approach of choice for removing large stones (> 12–15 mm).
When surgery is not an option and stones cannot be removed from the common bile duct by endoscopic methods alone, or when ERCP cannulation fails repeatedly, percutaneous transhepatic cholangiography can be used to facilitate access to the biliary tree through a rendezvous procedure. Targeted percutaneous lithotripsy can also be helpful, but oral dissolution therapy is only of historical interest because of its poor efficacy and safety.
In patients who are poor candidates for surgery, long-term biliary stenting by insertion of an endoprosthesis is a safe and effective alternative to duct clearance. However, periodic replacement of the stent to maintain patency is required for life. This approach should be used only in highly selected patients because of the risk of subsequent cholangitis due to clogging of the stent.40 Additional treatment with ursodeoxycholic acid or a choleretic agent has not been shown to improve rates of stone clearance.41
Do all stones require treatment?
Most of the studies of treatment strategies that we identified included patients with symptomatic common bile duct stones. The common practice is to remove common bile duct stones in patients presenting with symptoms. Indeed, most patients who are symptomatic will have recurrent symptoms if their condition is left untreated.42
This approach, however, may not work in the context of “silent” stones, which are now more frequently seen because of improved imaging techniques. Such stones are incidentally found in the common bile duct in the absence of jaundice, pancreatitis, and abnormal bilirubin and liver enzyme levels, and when the diameter of the duct is less than 8 mm on preoperative ultrasound.9 Because the majority of the literature has stemmed from common bile duct stones that have caused symptoms, common practice is to remove all stones detected in the common bile duct, as long as the patient can tolerate the proposed therapeutic procedure. The detection of possible silent stones remains controversial, and we suggest that only patients at intermediate or high probability of having a common bile duct stone be investigated. Such an approach would minimize the chance of detecting an asymptomatic stone. Many disparate data converge to support this recommendation.
Three randomized controlled trials involving patients with a low preoperative probability of common bile duct stones compared cholecystectomy alone and in combination with intraoperative cholangiography. Rates of detecting stones were 2%–12% in the cholangiography groups.43–45 However, at one year, the incidence of symptomatic retained stones did not differ significantly between the two groups.44,46 In another trial in which 280 patients were randomly assigned to these two treatment categories, an extended follow-up to eight years postoperatively found no significant difference in the incidence of adverse outcomes between the groups.9
Similar qualitative observations were made previously in a different context. In a cohort study that included 21 patients undergoing extracorporeal shockwave lithotripsy for gallstones, most (85%) of the stone fragments smaller than 8 mm and all of the fragments smaller than 3 mm passed through the common bile duct without causing symptoms.47 These findings suggest that silent stones can often pass spontaneously out of the common bile duct without causing symptoms. Further, in a study involving 997 consecutive patients undergoing routine intraoperative cholangiography at the time of laparoscopic cholecystectomy, the cholangiogram catheter was left in the cystic duct postoperatively in 46 patients with a filling defect in the bile duct found at operation, to allow two follow-up cholangiograms over six weeks postoperatively.48 Twelve of the 46 patients had possible false-positive cholangiograms, but more than one-third of the patients with filling defects at 48 hours passed the stones spontaneously within six weeks. Of the 22 patients (2.2% of the total study population) with persistent stones at six weeks after laparoscopic cholecystectomy, none was symptomatic, and the majority of the stones were cleared successfully by means of postoperative ERCP.
Changes in management
Several approaches to the management of common bile duct stones have evolved substantially over the last decade, warranting discussion. These include the use of routine intraoperative cholangiography, the choice of alternative imaging techniques other than routine intraoperative cholangiography, and cholecystectomy after endoscopic sphincterotomy (for discussions of these topics, see Appendix 6, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110896/-/DC1).
The management of gallstone pancreatitis, discussed in the following section, is one area that has changed substantially over the last few years.
Gallstone pancreatitis
Gallstones and microlithiasis are the most common causes of acute pancreatitis. In a prospective study involving 89 consecutive patients with acute pancreatitis, 20% were classified as having idiopathic pancreatitis after imaging with one or more of transabdominal ultrasonography, CT scanning and ERCP. Among these patients, 77.8% were found to have gallstones or microlithiasis on endoscopic ultrasonography.49
The timing of cholangiography and treatment in the management of gallstone pancreatitis has been of considerable debate, particularly for patients with severe acute pancreatitis. Three randomized trials showed that early ERCP with or without endoscopic sphincterotomy in patients with severe gallstone pancreatitis resulted in reduced morbidity.50–52 In contrast, other randomized trials showed that early ERCP did not result in reduced systemic or local complications53–55 except in patients with concomitant cholangitis.55 In one trial, early ERCP resulted in increased morbidity.53 Also, early surgery may lead to more unnecessary exploration of the common bile duct and increased mortality.56 In two meta-analyses involving a total of 717 patients from five trials, ERCP within 72 hours after presentation resulted in no improvement in the incidence of local pancreatic or overall complications, or mortality.57,58 We thus suggest that urgent ERCP in suspected gallstone pancreatitis be performed only when there is concomitant acute cholangitis or biliary obstruction (perhaps using a serum bilirubin level > 85.5 mmol/L as a cutoff value57). Otherwise, initial conservative management is favoured, with intraoperative cholangiography at the time of subsequent laparoscopic cholecystectomy.
Early elective cholecystectomy in patients with resolved gallstone pancreatitis is important to minimize recurrence. A randomized trial from the 1980s showed that delaying open cholecystectomy beyond six weeks after the resolution of gallstone pancreatitis was associated with recurrent symptoms and recurrent gallstone pancreatitis.59 This has been reconfirmed in the context of laparoscopic cholecystectomy.60 The performance of an endoscopic sphincterotomy is not protective against the recurrence of symptoms and complications.60,61
Conclusion
The management of common bile duct stones has undergone substantial evolution with the advent of accurate and safe methods of diagnosis and treatment. These advances have led to algorithms with safer treatment options and to the emergence of newer concepts such as the “silent” stone. Box 2 provides a fictional example of how to apply the results of this review in clinical practice.
Applying the results of this review in clinical practice (fictional case)
A 45-year-old woman reports a two-hour history of constant, severe pain in the right upper quadrant of her abdomen radiating to her back, with associated nausea. She has no fever, her pulse is 84 beats/min, and her blood pressure is 124/76 mm Hg. There is tenderness without guarding or rebound in the right upper quadrant of her abdomen. Laboratory investigation shows elevated levels of bilirubin (25 [normally 5–17) μmol/L) and γ-glutamyltransferase (70 [5–36] IU/L). Levels of alanine transaminase, aspartate transaminase, alkaline phosphatase and amylase were within normal limits. An ultrasound of the abdomen shows stones in the gallbladder and a slightly dilated (9 mm) common bile duct (the upper limit is 6–8 mm, increasing with age or a history of cholecystectomy).
This patient has an intermediate probability of having a common bile duct stone based on the prediction model proposed by Barkun and colleagues.15 A noninvasive method for cholangiography should be chosen, preferably magnetic resonance cholangiopancreatography. Endoscopic retrograde cholangiopancreatography (ERCP) is an option depending on the local resources and expertise. If a stone is detected, and again based on local expertise, preoperative ERCP, or laparoscopic clearance of the bile duct, should be performed in addition to laparoscopic cholecystectomy.
Any contemporary approach to the management of common bile duct stones must take into consideration the availability of local expertise and technology. An integrated health care team including surgeons, gastroenterologists and radiologists will help to decrease patient morbidity, enhance cost-effectiveness and optimize patients’ quality of life.
Key pointsThe management of patients suspected of having stones in the common bile duct depends on whether their probability of having such stones is high, intermediate or low.
Most people who present with symptomatic common bile duct stones will have recurrent symptoms if the stones are left untreated.
The investigation of possible “silent” stones remains controversial, because such stones may pass spontaneously without causing symptoms.
Common practice is to remove all detected common bile duct stones, as long as the patient can tolerate the proposed therapeutic procedure.
Footnotes
Competing interests: Alan Barkun has received consultancy fees from Takeda Canada and Olympus, and speaker fees from AstraZeneca Canada, Takeda Canada and Sanofi-Aventis, conducted research sponsored by grants from Cook and Boston Scientific, and has received payment from AstraZeneca Canada for the development of educational presentations. No competing interests declared by Majid Almadi or Jeffrey Barkun.
This article has been peer reviewed.
Contributors: All of the authors contributed substantially to the conception and design of the study, the acquisition and interpretation of data, and the drafting and critical revision of the manuscript. All of the authors approved the final version of the manuscript submitted for publication.
References
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

