


A 33-year-old woman who was 21 weeks pregnant presented at the emergency department with symptoms of nausea and vomiting. On examination, she had epigastric discomfort. Shortly after admission, she collapsed and cardiac arrest occurred. Advanced life support was provided immediately. After endotracheal intubation, unilateral excursions of the right lung were noted. Right endobronchial intubation was excluded after thorough auscultation of the lung and gradual retraction of the tube. Acute tension pneumothorax was suspected, and emergency thoracentesis1 was performed at the second intercostal space on the left with an 18-gauge needle, draining some clear fluid. Ventilation of the left lung remained impossible. Transthoracic echocardiography showed a shift of the heart to the right. A surgeon introduced a 28-Charrière thoracostomy drain at the fourth intercostal space, midaxillary, which evacuated 400 mL of clear fluid. Return of spontaneous circulation was achieved shortly afterward. A computed tomographic scan showed a large gastrothorax with shift of the mediastinum to the right (Figure 1A). Placement of a nasogastric tube drained another 1500 mL of gastric content, resolving the tension (Figure 1B); however, echocardiography of the fetus showed no heart activity.
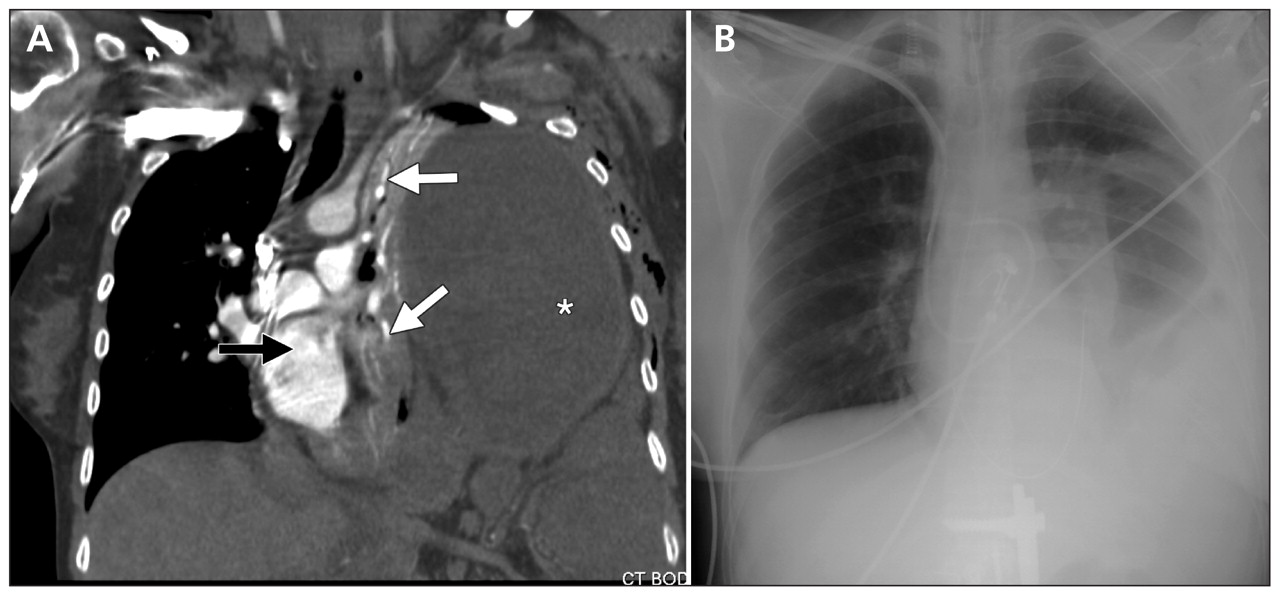
(A) Computed tomographic scan of the thorax in the coronal plane in a 33-year-old woman, taken after resuscitation. A mediastinal shift to the right is seen (black arrow), with the left lung completely compressed (white arrows) by gastrointestinal viscera. (*Intrathoracic stomach.) (B) Radiograph of the thorax showing resolution of the mediastinal shift by nasogastric decompression. Gastrothorax is still visible.
Diaphragmatic hernias have a low incidence,2,3 but they can become life-threatening and require emergency treatment when abdominal viscera herniate through the diaphragm. Because of the low incidence and the mimicking of a tension pneumothorax,4 the diagnosis may be delayed or even missed. Decompression using a naso- or orogastric tube remains the best treatment in this situation.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

