


Three weeks after an elective total abdominal colectomy for refractory ulcerative colitis, a 45-year-old woman presented to the emergency department with increasing abdominal pain. Her operation and immediate postoperative course had been unremarkable, but within days of discharge she had developed increasingly severe abdominal pain. She had no symptoms of sepsis or nausea. Her ileostomy continued to function well.
On examination, her abdomen was soft without signs of peritonitis. Her pain was substantially out of proportion to her benign clinical examination. Routine laboratory values showed mild leukocytosis (leukocyte count 13.6 [normal 4.5–11.0] × 109/L) and were otherwise within normal limits. Computed tomography of the abdomen showed enlargement of the superior mesenteric vein with a prominent intraluminal clot (Figure 1). The diagnosis of acute superior mesenteric venous thrombosis was made.
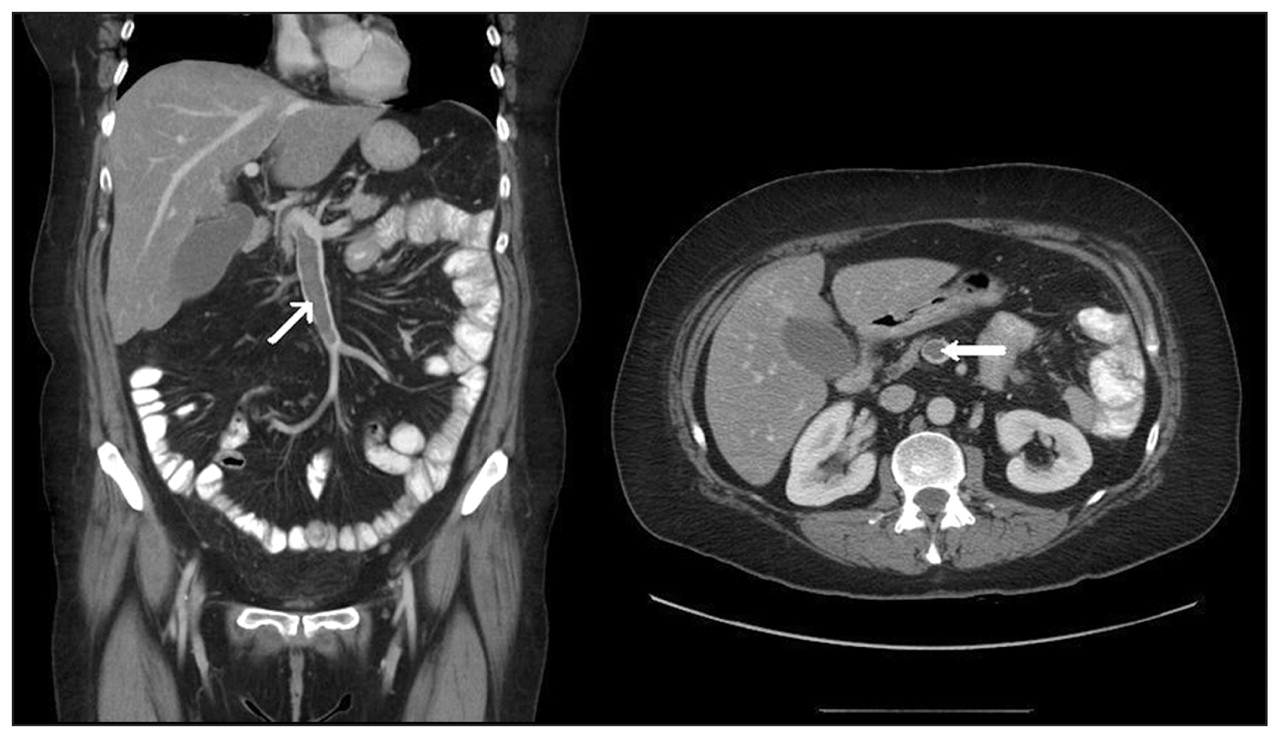
Coronal and axial views of a computed tomographic scan of the abdomen of a 45-year-old woman showing enlargement of the superior mesenteric vein, with well-defined enhancement of the vascular wall. An intraluminal clot is seen (arrows), showing extensive thrombosis of the superior mesenteric vein.
Acute mesenteric venous thrombosis is an uncommon condition. Acute insufficiency of mesenteric arterial blood flow accounts for 60%–70% of instances of mesenteric ischemia, with mesenteric venous thrombosis occurring in only 5% of instances.1 Although colicky abdominal pain is a common presenting complaint, patients with mesenteric venous thrombosis may be asymptomatic or may present with peritonitis if intestinal ischemia has developed. Outcomes of this condition include bowel infarction, hemorrhage, sepsis and death. A high index of suspicion is required. The most common etiologies include prothrombotic states such as congenital coagulation disorders, paraneoplastic syndromes, intra-abdominal inflammatory conditions (e.g., sepsis, pancreatitis, inflammatory bowel disease, diverticulitis), the postoperative state, cirrhosis and portal hypertension.2
There are no formal guidelines for the treatment of mesenteric venous thrombosis: the clinical status of the patient guides the initial management. If the patient is clinically unstable, immediate abdominal exploration with resection of infarcted bowel is warranted. For clinically stable patients, early systemic anticoagulation is appropriate to halt the spread of the thrombus. Mechanical thrombectomy may be considered if a contraindication to anticoagulation exists. Depending on local expertise, site-directed thrombolytic therapy may be used.3 The duration of anticoagulation therapy depends on the suspected etiology of the thrombosis and may involve 6 to 12 months’ to life-long therapy.
In our patient, systemic anticoagulation was started immediately, and she made a complete recovery.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

