


Case
[The following is a fictitious case based on experience with similar cases.]
Debby is a 45-year-old woman with a self-detected palpable breast lump noticed incidentally one week ago. The lump is tender and increasing in size. Her sister was diagnosed with breast cancer at age 48. Debby is terrified that this may be cancer.
About 1 in 10 women who present with a new breast lump has breast cancer. 1 The younger the age of the patient at presentation, the less likely the lump will prove to be cancer. Only 1 in 100 women with a new breast lump at age 40 or younger will have breast cancer. 2 Because 10% of malignant lesions in young women have features consistent with a fibroadenoma, 3 new palpable masses in women of any age should be thoroughly evaluated. Cysts account for about 25% 4,5 of all breast lumps and are common in premenopausal women over 35 years of age and uncommon in postmenopausal women unless they have received hormone therapy. 6 In this article, we review an approach to the initial management of palpable breast lumps and describe several techniques for breast lump aspiration in the outpatient setting.
Evidence
Most information on managing breast lumps is from cohort studies. There are several algorithms available for the diagnosis of a breast lump. 1,7–9 The 1998 consensus guideline from the Department of Surgery at the University of Toronto is particularly useful for family physicians in an office setting. 8 It was updated in 2009 by a group of experts in the management of breast lumps — including four surgical oncologists (DM), a radiologist, a pathologist, a general practitioner-oncologist (RH) and a nurse practitioner —using a review of the literature since the original algorithm was developed (Figure 1). It is applicable to all postpubescent women with a discrete palpable lump that is not suspicious for cancer.
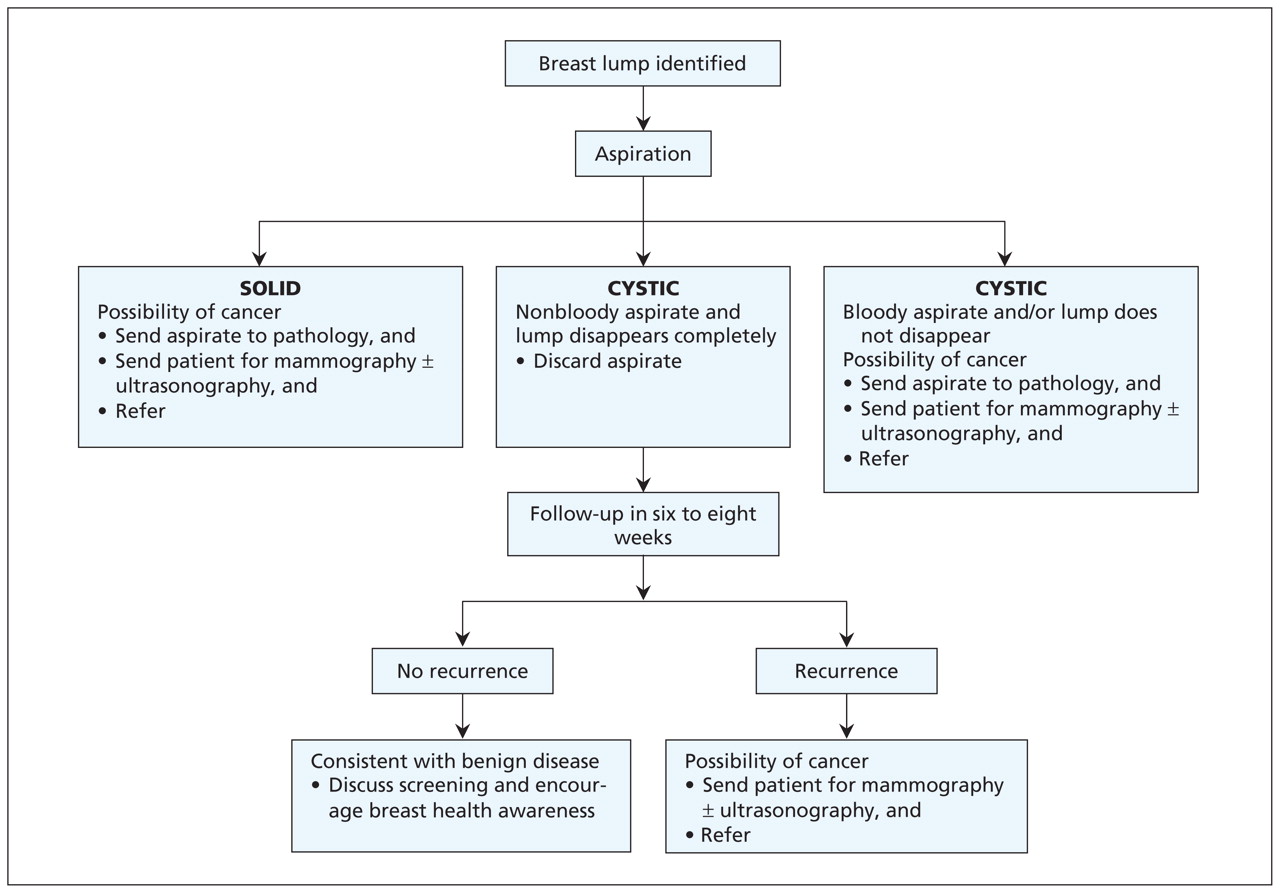
Figure 1: Consensus guideline for in-office aspiration of a discrete palpable breast lump that is not suspicious for cancer. Adapted, with permission, from Can Fam Physician 1999;45:1928. 8
Initial management
A patient presenting with a lump and features suggesting cancer (e.g., hard irregular mass fixed to the skin, palpable ipsilateral nodes or peau d’orange) should immediately be sent for mammography, ultrasonography and core biopsy, and referred to a breast surgeon.
Lumps that are not clinically suspicious for malignancy can be managed initially in the family physician’s office. The algorithm (Figure 1) advocates fine-needle aspiration of palpable lumps and assumes access to a skilled cytopathologist.
Even an experienced examiner can find it difficult to differentiate between cystic and solid lesions by palpation alone. Imaging can be useful, but the wait time may result in unnecessary anxiety for the patient. Some studies support the initial use of aspiration or ultrasound to differentiate between cystic and solid lesions. 1,9 Ultrasound is 98%–100% accurate in identifying simple cysts, but initial in-office aspiration of a cyst is therapeutic, immediately diagnostic and more cost-efficient. 1 If the physician or patient is not comfortable with breast lump aspiration, ultrasound is an alternative initial approach to determine whether the lump is cystic or solid. 1,9
Case continued
Examination showed a tender fluctuant mass measuring 2 cm in the upper outer quadrant of the right breast. Debby had no overlying skin changes or supraclavicular or axillary adenopathy.
Aspiration of a breast lump
Aspiration is a quick and straightforward initial approach for patients with a breast lump and no features suggestive of cancer. It can be done in the family physician’s office for all women with a discrete palpable mass who do not have breast implants and who are not on anticoagulants. There is no need for a local anesthetic before aspiration.
Two common approaches are described in Boxes 1 and 2. 8,10,11 Aspiration can also be practised with a model of a breast lump (Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.090416/DC1). 12

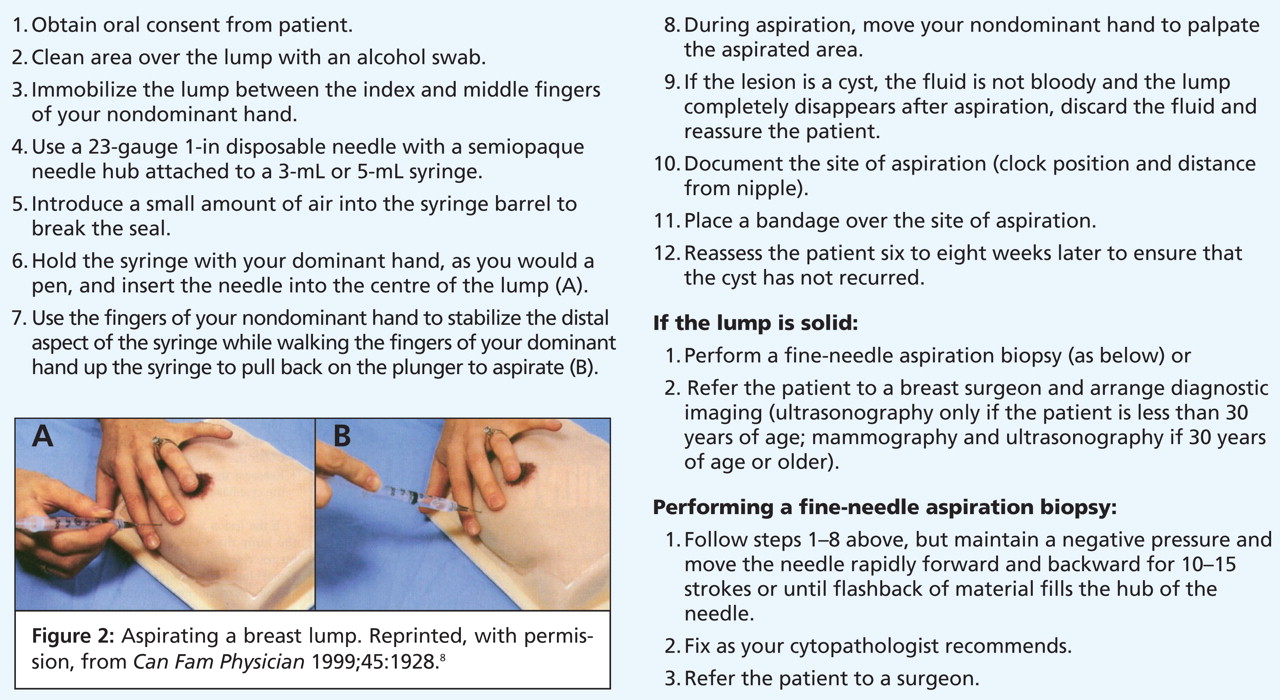
Box 1: Technique for aspirating a breast lump 8 (Figure 2)
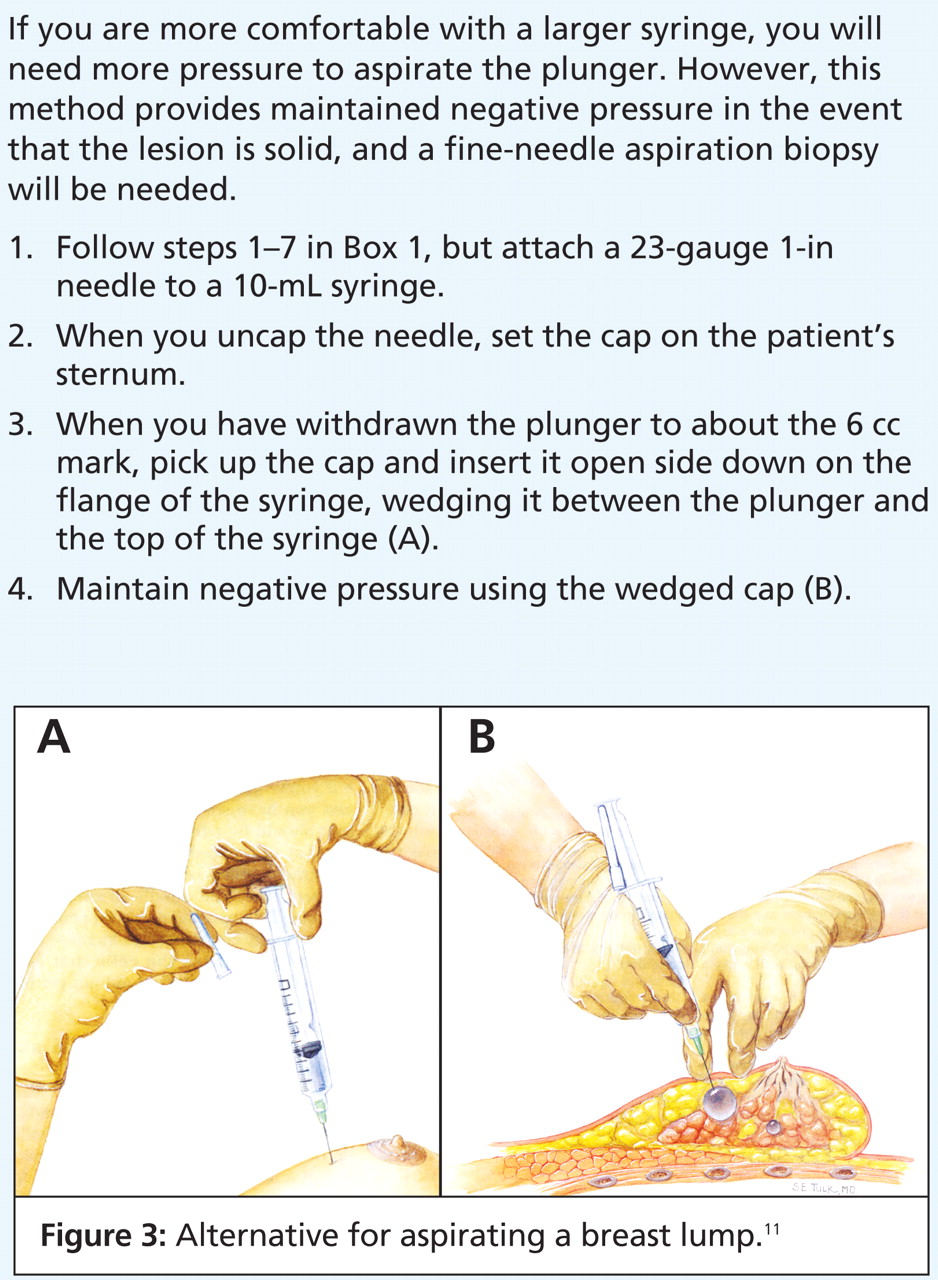
Box 2: Alternative technique (more difficult) for aspirating a breast lump 10 (Figure 3)
If the lump completely disappears with the aspiration of nonbloody fluid, the lesion is a simple cyst, and the fluid may be discarded. 13 The cyst’s location in the breast should be documented precisely (e.g., clock position and distance from the nipple).
The finding of bloody aspirate, a lump that does not completely disappear or a lump that recurs warrants referral to a surgeon. The aspirated fluid should be sent for pathologic examination. Any of these features may be associated with cancer; however, only 0.5%–1.0% of women presenting with a palpable cystic lesion will have an associated underlying neoplasm. 6,14
If the lesion is solid, a fine-needle aspiration biopsy could be performed, or the needle could be removed without further aspiration. Any specimen obtained should be fixed as per the local laboratory’s policy and sent for analysis by a cytopathologist.
Complications of aspiration include discomfort at the site of aspiration, bruising if there is inadvertent puncture of a vessel, infection, vasovagal response (which usually resolves quickly after the needle is removed) or, uncommonly, a pneumothorax. 8 If air is drawn into the syringe, immediate inspiratory and expiratory chest radiographs should be taken. Pneumothorax is unlikely if lesions close to the chest wall are moved over a rib before aspiration. 8
Aspiration does not increase the rate of false-positive results of mammography provided that the radiologist is advised about the site of aspiration. 15 If the lump proves to be cancerous, there is no evidence that a needle biopsy will cause the tumour to spread. 16 In fact, most cancers are diagnosed by a needle or core biopsy before surgery.
Further investigations
In the case of a simple cyst that resolves with aspiration, the patient should be seen six to eight weeks later to determine whether there is a recurrence of the cyst. 14 If the cyst recurs, the patient should be sent for mammography or ultrasonography, or both, and be referred to a surgeon for further assessment. If the cyst does not recur, additional tests are not necessary. This is, however, a good opportunity to ensure that screening tests are up to date.
If the lesion is solid, the patient should be sent for imaging and referred to a surgeon. If the patient is less than 30 years of age, only ultrasonography is recommended; for women 30 years of age or older, both mammography and ultrasonography should be ordered. 17 A triple assessment (examination, imaging and aspiration) to diagnose solid breast lumps ensures concordance between the clinical findings and the results of imaging and pathologic examination. 18 Although some clinicians elect to monitor palpable, presumed fibroadenomas without cytopathologic testing, this approach will miss some breast cancers in young women. In this group, most delays in the diagnosis of breast cancer result from falsely reassuring clinical findings or imaging results. 19
Case outcome
Debby’s breast lump disappeared completely after aspiration of clear fluid. She was relieved to know that the lump was only a cyst. She promised to return to the office in six weeks for a breast examination. Debby was offered mammography because she was 45 years old and had a first-degree relative with premenopausal breast cancer. However, because she had undergone mammography within the last year, there was no need for additional investigations at this time.
-
Aspiration of a palpable breast lump allows immediate reassurance for women with breast cysts and timely investigation and referral for women with solid masses.
-
If the lump is a cyst, the aspirated fluid may be discarded provided the fluid is not bloody and the lump disappears.
-
If the lump is solid, triple assessment (clinical examination, breast imaging and fine-needle aspiration cytologic assessment) is warranted.
Key points
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: None declared.
Contributors: Both authors contributed to the development, writing and review of the article, and both approved the final version submitted for publication.
Acknowledgements: The authors thank Dr. K. Bukhanov, Dr. T. Cil, Dr. W. Leong, B. Lord, Dr. M. Reedijk and Dr. B. Youngson for their assistance in updating the consensus guideline in Figure 1.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

