


The case
Emma is a 38-year-old woman who has had asthma since infancy. She was occasionally admitted to hospital in childhood, but her asthma became less troublesome in adolescence. She continued to need regular maintenance therapy with low-dose inhaled corticosteroids. She reported a marked worsening of her symptoms after the birth of her first child. In the past 3 years, she has used inhaled combination therapy in the form of fixed-dose salmeterol (50 mg) and fluticasone (500 mg), taken twice daily, and has still needed quick-relief bronchodilators on average 2 or 3 times per day. She awakens with asthma symptoms about once a week and is unable to participate in fitness classes because of wheezing.
Over the past year, Emma has had 4 exacerbations for which prednisone therapy was required. One of the exacerbations was sufficiently severe to require a visit to an emergency department, but she was not admitted to hospital. At that point she was referred by her family physician to an asthma centre for further review.
The total cost of asthma in Canada has been estimated at more than $500 million annually. 1 The substantial financial burden of this disease is directly linked to the failure to achieve control of the disease. Costs also increase significantly with disease severity: a small cohort of severely ill patients consumes 80% of all asthma-related health care resources. 2,3 Inadequately controlled asthma accounts for more than three-quarters of related emergency department visits, admissions to hospital and unscheduled consultations with a physician, resulting in an estimated cost of $162 million per year in Canada. 4,5
Central to the management of asthma is the assessment of disease control. This is accomplished by determining the frequency of the patient’s daytime and nighttime symptoms, the need for quick-relief bronchodilator therapy, limitations to physical activity, occurrence of exacerbations, and absence from work, school or usual activities. In addition to these symptom-based parameters of control, physicians should measure lung function when the patient is thought to be optimally treated. 6 This will determine whether the forced expiratory volume in 1 second (FEV1) or peak flow is normal or nearly so. These parameters are then used to categorize the patient’s asthma as being controlled, partly controlled or uncontrolled, 6 as described in an earlier article in this series. 7
Sources of information
To identify relevant articles on omalizumab and other therapies for difficult-to-treat asthma, we performed a literature search of the “Asthma and Wheez*” register of the Cochrane Airways Group, which was originally created through a comprehensive search of EMBASE, MEDLINE and CINAHL. We searched all of the register’s original research studies and reviews using the following search terms: “severe asthma,” “omalizumab” and “Xolair.” The current review encompasses records published in or added to the register between 2005 and June 2008. Of 783 articles retrieved, 50 were in English and provided nonduplicative clinical trial data or case reports on human asthma, adverse events, and the efficacy and safety of omalizumab and other standard and non-traditional treatments. Articles describing the use of omalizumab and other treatments for indications other than asthma were not reviewed, except for sections reporting adverse events. We performed a supplementary literature search using the following search terms: “asthma” with publication date from 2005 to 2008 and “omalizumab OR Xolair OR methotrexate OR MTX OR gold OR cyclosporin OR macrolide OR clarithromycin OR troleandomycin OR erythromycin OR josamycin OR azithromycin OR roxithromycin OR IVIG OR immunoglobulin OR immunoglobulin OR immune globulin OR thermoplasty OR Alair OR etanercept OR Enbrel OR TNF-α OR TNF alpha OR necrosis.” We included relevant articles from among those identified by this supplementary search (n = 184) in the current publication. We performed a further supplementary literature search using the following search terms: “asthma” with publication date from 1999 to 2009.
We based our grades of evidence on those of the Canadian Task Force on Preventive Health Care, 8 as detailed in a previous article in this series. 9
Asthma control, severity and unresponsiveness
For the majority of patients with asthma, control can be achieved with conventional therapy, and indeed some patients enjoy complete freedom from asthma symptoms using such therapy. 10,11 Unfortunately, surveys in Canada and elsewhere have shown that many patients, perhaps the majority, fail to achieve adequate disease control. 4,12 It is widely believed that this is not a consequence of intrinsically severe asthma, but rather of inadequate management, poor patient education or a combination of these 2 factors. 4,13
A separate issue from symptom control is the definition of asthma severity. 6,14 Frequent symptoms and exacerbations are not synonymous with severe disease. Patients with mild disease may have frequent symptoms or exacerbations if adequate maintenance therapy has not been prescribed or they are not taking their prescribed medications. Conversely, patients with severe disease may be free of symptoms and exacerbations if they have been given appropriate therapy. A simple guide to a patient’s degree of asthma severity is the minimum amount of medication that he or she needs to maintain disease control. 15
Asthma severity may change over time. Thus, it is incumbent upon physicians to reassess control regularly. Such follow-up should occur every 6 to 12 months, depending on the severity of symptoms. 15 For some patients, there is no response to usual therapy. Some have no response at all to quick-relief bronchodilators or inhaled corticosteroids, whereas for others, these conventional therapies are only partially effective. Patients with these forms of refractory or difficult-to-control asthma usually receive increasingly large doses of inhaled corticosteroid with adjunctive agents but do not attain the desired levels of disease control. Ultimately, such patients are often given systemic corticosteroids, either frequently or continuously, to control or at least blunt the most severe manifestations of the disease. In this review, we consider management strategies for patients with difficult-to-treat asthma.
Confirming the diagnosis
Evaluation of patients with difficult-to-treat asthma should begin with confirmation or reconfirmation of the diagnosis. A long history of disease does not in itself confirm the presence of asthma, nor does it rule out the subsequent development of cardiac or nonasthma pulmonary disease. The diagnosis of asthma requires the presence of compatible symptoms plus pulmonary function tests showing variability of airflow obstruction.
The possibility of other conditions must also be considered. Airflow obstruction that is persistent and unresponsive to bronchodilator raises the possibility of a nonasthmatic obstructive lung disease such as chronic obstructive pulmonary disease 16 or bronchiolitis obliterans. Moreover, a lack of change in airflow obstruction either over time or with more aggressive therapy increases the likelihood of such diagnoses.
Pulmonary function testing may also hint at other diagnostic possibilities. Flattening of the flow–volume loop on either the inspiratory portion or the expiratory portion or both would suggest the presence of vocal cord dysfunction. Inappropriate closure of the vocal cords on inspiration may be deliberate or unconscious and may result from vocal cord irritation. 17 These problems of the vocal cords may be difficult to diagnose, and their true prevalence may be underestimated by researchers.
Plain chest radiography has little utility in the routine assessment of asthma but is helpful in ruling out other illnesses that may cause symptoms of dyspnea or cough, such as congestive heart failure.
The case continued
A specialist at the asthma centre interviews Emma and gathers the following detailed history. The patient is a lifetime nonsmoker, and no one in her household smokes. She works in a sales office where she is not exposed to any obvious occupational respiratory hazards. However, each spring she suffers from seasonal allergic rhinitis, which she treats with antihistamines or nasal corticosteroids. She does not have any pets. She experiences gastroesophageal reflux only rarely. The results of the physical examination are unremarkable except for both pallor and edema of the nasal mucosa and expiratory wheezes heard throughout the lungs. Reproducible spirometry indicates that FEV1 is 52% of predicted before and 67% of predicted after administration of inhaled bronchodilator. Additional pulmonary function testing reveals moderate gas trapping and normal diffusion capacity. Chest radiography shows flattening of the hemidiaphragms, but the results are otherwise unremarkable. Allergy skin-prick testing shows moderate (3+) reactions to dust and dust mite antigens and small (2+) reactions to tree and grass pollen and cat antigens. A certified asthma educator reviews the patient’s inhaler technique and her general knowledge about asthma. Subsequent review of pharmacy records and inspection of the patient’s inhalers are compatible with adherence to prescribed therapy.
Previous trials of adjunctive oral theophylline and mon-telukast and a trial of increased inhaled corticosteroid (i.e., fluticasone 500 μg twice daily in addition to salmeterol [50 mg] and fluticasone [500 mg] twice daily) did not alter Emma’s symptom pattern. Her family physician subsequently gave her a prescription for prednisone 15 mg daily, which resulted in partial relief of symptoms, a reduction in the need for short-acting bronchodilator to just one puff per day and improvement in prebronchodilator FEV1. However, her post-bronchodilator obstruction has persisted.
Addressing nonpharmacologic aspects of care
As outlined in previous Canadian consensus guidelines for the management of asthma, 15 it is essential that all patients receive appropriate asthma education. Surveys of Canadians with asthma have revealed that many lack a rudimentary understanding of their medications and often confuse reliever medications with preventive medications. 13 Furthermore, few have seen a certified asthma educator, and the vast majority do not have written action plans to guide management of exacerbations. 14 Most rely on physicians or pharmacists to answer their questions about asthma, but the time and resources available for such counselling are often limited. 13 Many patients have poor inhaler technique and hence fail to achieve control of their disease. 18 Comprehensive education must include not only information about appropriate use of medications, but also the teaching and assessment of optimal inhaler technique. Even the simple-to-use dry powder inhalers can be mishandled. In addition, it is important to evaluate whether environmental factors in patients’ homes or workplaces may be worsening their asthma symptoms.
Given all of these factors, hidden noncompliance may be a major factor in apparently difficult-to-control asthma. 19 Pharmacy records may be helpful in estimating consumption of prescribed medication. In addition, physicians or other members of the health care team may find it useful to explore with patients their concerns about using the medications, their health beliefs, the affordability of the drugs and other common barriers to medication usage. Health care providers might also inspect a patient’s inhalers to determine the prescription date and ask about the frequency of inhaler replacement to assess how often they are using inhaled controller therapies. 20 Strategies to improve compliance include education, use of treatment regimens that permit a reduced dosing frequency and use of combination therapy in a single inhaler. 21,22
In the home, dust mites are ubiquitous and many patients with asthma are skin-test positive to dust mite antigen. Pet dander is also an important factor in producing asthma instability. Patients who are allergic to pet dander often experience worsening of asthma during the winter months, when they spend more time indoors with their pets. The workplace is another primary source of substances that induce or worsen asthma. An estimated 10% to 20% of adults with asthma are exposed to such substances at work. 23 Hence it is vital that the health care professional take an allergy history. Allergy skin-prick testing will provide complementary information.
Managing comorbid conditions
Treating chronic nasal diseases is often helpful for asthma control. The simple addition of a nasal corticosteroid often improves asthma control in patients with allergic rhinitis, which is often overlooked in the context of asthma. 24 Oral antihistamines have no role in the management of asthma. However, they can be used either intermittently or regularly as monotherapy in the treatment of mild allergic rhinitis or in addition to nasal inhaled corticosteroids in moderate to severe allergic rhinitis that is incompletely responsive to nasal inhaled corticosteroids. 25 The role of treating gastroesophageal reflux disease in the management of asthma is not clear; however, for patients with troublesome asthma who suffer more than occasional reflux symptoms, convincing reports have shown reduced frequency of exacerbation with use of antireflux therapies such as proton pump inhibitors. 26 Obesity has been linked with a suboptimal response to inhaled agents and difficult-to-control asthma, but the nature and clinical implications of the association are unclear. 27
Screening for asthma-associated syndromes
When asthma is difficult to treat and airflow obstruction persists after therapy, special diagnostic tests may help to determine the cause. For example, α1-antitrypsin deficiency is not uncommon in white populations and predisposes affected people to the development of premature emphysema. 28 This early-onset obstruction is commonly misdiagnosed as asthma. The average delay between the onset of symptoms and the correct diagnosis of α1-antitrypsin deficiency is about 10 years.
Patients with asthma who require oral steroids frequently or continuously may have one of the asthma syndromes in which this pattern is common. Allergic bronchopulmonary aspergillosis is reported to be present in about 13% of people who present to asthma clinics, 29 although its prevalence in the population has not been clearly established. This disease is characterized by difficult-to-control asthma, with frequent exacerbations, in the presence of chronic colonization by Aspergillus and a characteristic immunologic response to the fungus. Patients will typically have proximal mucous plugging and tenacious sputum. Proximal (central airway) bronchiectasis may result. Laboratory tests may reveal the presence of Aspergillus in sputum, while positive immediate skin-test responses plus positive delayed responses would suggest the dual-phase immunologic response (types I and III). Serum precipitins are typically positive for Aspergillus.
Churg–Strauss vasculitis is another variant of asthma in which steroid dependence is typical. 30 Before development of a vasculitic lesion of the skin or lung, an underlying vasculitis may be revealed by appropriate immunologic studies such as measurement of the titre of antineutrophil cytoplasmic antibody. In a recent population-based study, this antibody was estimated to have incidence rates of between 0 and 75 per million person-years among individuals with asthma. 31
Some patients appear to have resistance to systemic corticosteroids, as demonstrated by a lack of clinical improvement with high doses of systemic steroids. Other patients have disease that is responsive to systemic steroids and show clinical improvement when these medications are administered, but their condition becomes unstable when the drugs are withdrawn. These 2 groups of patients have asthma that is described as steroid-resistant and steroid-dependent, respectively. In vitro assays have been used to define corticosteroid receptor responsiveness. However, such assays are not widely available, and the response to steroids is usually assessed clinically instead. Importantly, noncompliance with recommended oral steroids can confound such assessments; therefore, depot steroids are recommended for assessing responsiveness to steroids. 32–34
Many patients with deficiency of either immunoglobulin G2 or specific polysaccharide antibody have recurrent respiratory conditions, such as bronchiectasis, bronchopneumonia, bronchitis, obstructive lung disease and hyperreactive airways, any of which may present as “asthma.” 35
The case continued
Several laboratory tests and other investigations are requested for Emma. Her complete blood count is normal, with no eosinophilia. The serum α1-antitrypsin level is lower than normal: 0.71 (normal range 0.8 to 1.9) g/L. Follow-up testing reveals an MZ phenotype, confirming that she is a heterozygote (carrier) for the deficiency, but with serum levels adequate to protect against premature development of emphysema. As such, no specific therapy is required. Serum levels of immunoglobulins A, G and M are normal, as is immunoglobulin E (120 IU/mL). The erythrocyte sedimentation rate is not elevated. Tests for antineutrophil cytoplasmic antibodies and serum precipitins to common fungi, including Aspergillus spp., are negative. Sputum induction is unsuccessful. Computed tomography of the chest shows thickening of medium-sized airways and scattered nonspecific nodules, with no evidence of bronchiectasis or emphysema.
Monoclonal anti-immunoglobulin E therapy
Omalizumab is a humanized mouse monoclonal antibody that binds to circulating immunoglobulin E, thereby rendering this moiety inactive. 36 In clinical trials, omalizumab reduced symptoms and exacerbation rates among patients with atopic disease whose asthma was uncontrolled by moderate- or high-dose inhaled corticosteroids with or without adjunctive long-acting β2-agonist therapy. Omalizumab should be dosed according to pretreatment serum total immunoglobulin E level and body weight, using a specified dosing table. It should be administered subcutaneously, under medical supervision, either biweeky or monthly in a clinic setting.
The majority of adverse events associated with omalizumab are minor. 37 The most common dermatologic adverse events are pruritus (2%) and dermatitis (2%). The most common respiratory adverse effects are upper respiratory tract infection (20%), sinusitis (16%) and pharyngitis (11%). The most common nervous system adverse events include headache (15%) and dizziness (3%). The musculoskeletal adverse effects include arthralgia (8%), fracture (2%), leg pain (4%) and arm pain (2%). Local adverse effects related to reactions at the injection site occur in 45% of patients and include bruising, redness, warmth, burning, stinging, itching, hive formation, pain, indurations, development of a mass and inflammation. 37
Reports indicate that anaphylaxis occurs in 0.09% to 0.2% of people after administration of omalizumab. 37,38 The majority of cases occur within 2 hours of administration of the medication and are most likely to occur after the first few doses. Thus the injections must be given in a medically supervised setting, with postinjection observation, and the health care providers administering the drug should be prepared to manage anaphylaxis, which can be life-threatening. 38 There have been recent reports of anaphylaxis onset 2 to 24 hours or even longer after omalizumab treatment. 39,40 Hence, patients should be informed of the signs and symptoms of anaphylaxis and instructed to seek immediate medical care should this problem occur.
Omalizumab costs $1200 to $2400/month ($600 for a 150-mg vial). The cost-effectiveness ratio has been determined to be at least $63 000 per quality-adjusted life year, and possibly in excess of 10 times more than this. 41,42 Therefore, there is considerable debate about its cost–benefit ratio. The cost can be a particular barrier for patients who have no private health insurance. The province of Quebec has reimbursed patients for the cost of omalizumab under its Exceptional Patient Program since September 2005. Governments in many European countries, the United States and the United Kingdom also reimburse patients for omalizumab. A committee of the UK National Health Service’s National Institute for Health and Clinical Excellence concluded in 2007 that, for a narrowly defined group of people who are severely affected by asthma, use of omalizumab as add-on therapy can be cost-effective, provided that therapy is discontinued after 16 weeks if there is no response and that vial wastage is minimized. 43
Omalizumab therapy should be considered for patients with severe asthma who require frequent or constant oral steroids despite continuous therapy with inhaled steroids and adjunctive therapy and who meet the criteria listed in Box 1. 44,45 Very high levels of serum immunoglobulin E preclude treatment with omalizumab; in such patients, it is impossible to administer sufficient monoclonal therapy to bind more than 95% of the circulating immunoglobulin and hence have an effect.

Before therapy with omalizumab is initiated, the patient should be assessed by a specialist. The response to omalizumab should be evaluated at 6 months and therapy discontinued for those who have not benefited. There is currently insufficient evidence to recommend omalizumab therapy for children with asthma (less than 12 years of age).
Other therapies for severe asthma unresponsive to usual care
Many other therapies have been used to treat severe or refractory asthma (Table 1). 46–89 However, none of them is currently considered a well-established therapy that can be recommended at this time. Several such interventions were tested in an era when higher-dose inhaled corticosteroid therapy with or without long-acting β2-agonists was not available; as such, positive findings from older studies are of questionable relevance in contemporary practice. Methotrexate, gold and cyclosporin A have corticosteroid-sparing effects clinically that must be weighed against a serious adverse effect profile. 46–54 For example, low-dose oral methotrexate therapy, widely used in the treatment of rheumatologic diseases, has been reported to reduce the need for systemic corticosteroids in severe asthma, but study results have been inconsistent. 46–50 A few patients have been reported to benefit from oral gold therapy, 53,54 and intravenous immunoglobulin has been reported to be of benefit, but only in uncontrolled studies. 55–59
Table 1: Other treatments for severe asthma
Dapsone 60 and hydroxychloroquine 61 also have not shown robust effects in studies. A relatively new treatment, the interleukin-5-blocking monoclonal antibody mepolizumab, is showing promise in preliminary randomized studies, but large randomized trials have not yet been published. 62–66 An interleukin-12-blocking agent has not yet shown efficacy against severe asthma. 67
Other studies have examined whether antibiotics have a role to play in the treatment of refractory asthma. For example, troleandomycin has been reported to reduce the need for oral steroids in patients with oral-steroid-dependent asthma, but is thought to do so by altering the metabolism of the oral steroids. 90
In the contemporary literature, conflicting findings have been reported for the use of antitumour necrosis factor α drugs such as etanercept or infliximab. 91 Further study is required.
Bronchial thermoplasty is a recently developed invasive procedure performed during serial bronchoscopic sessions, each lasting about 30 minutes, in which radiofrequency ablation is used to destroy bronchial smooth muscle, with the goal of reducing airflow variability. 68 The procedure is accompanied by a short-term increase in cough and wheeze, but over the ensuing weeks and months, patients with moderate to severe asthma experience improvement in various asthma outcomes. 69–71 However, respirologists and primary care physicians who treat patients with refractory asthma are awaiting results from long-term, controlled trials in patients with more severe or difficult-to-treat asthma. The intervention is currently not available outside of clinical trials.
Several therapeutic agents are under development for mild, moderate, severe and refractory asthma. In particular, specific target sites are being studied for the subsequent development of novel drug classes. The identification of ADAM33 (a disintegrase and metalloprotease 33 gene) as a major risk factor in the pathogenesis of bronchial hyperresponsiveness and airway wall remodelling provides insight into the pathogenesis of asthma and represents a novel therapeutic target for drug development. 92
Many patients with severe asthma also turn to alternative medicine. The approaches range from chiropractic to breathing exercises. There is a paucity of studies of these treatments, but to date the evidence indicates that none are efficacious (Table 1). 72–89
Outcome of the case
Emma is treated every 4 weeks with supervised omalizumab injections at a dosage estimated from the treatment monograph on the basis of her weight (70 kg) and initial immunoglobulin E level: 2 subcutaneous injections of 150 mg each for a total of 300 mg at each visit. After 3 months of this therapy, Emma is no longer experiencing exacerbations. The dosage of prednisone is reduced to 10 mg per day, although the patient continues daily use of a quick-relief bronchodilator. After 3 more months, she uses bronchodilator relief no more than twice weekly and no longer uses prednisone. Spirometry shows only mild airflow limitation and reveals that the level of gas trapping has been reduced.
Conclusions
The key messages for the management of uncontrolled asthma are presented in Box 2. The approach to and management of severe asthma is a complex process best implemented in specialized centres. Fortunately, although rates of morbidity and utilization of health care services are high, the number of people with very severe or difficult-to-treat asthma in Canada is relatively small. Currently, omalizumab seems to be a safe, well-tolerated addition to the armamentarium for suitable, carefully selected patients with severe, atopic asthma.
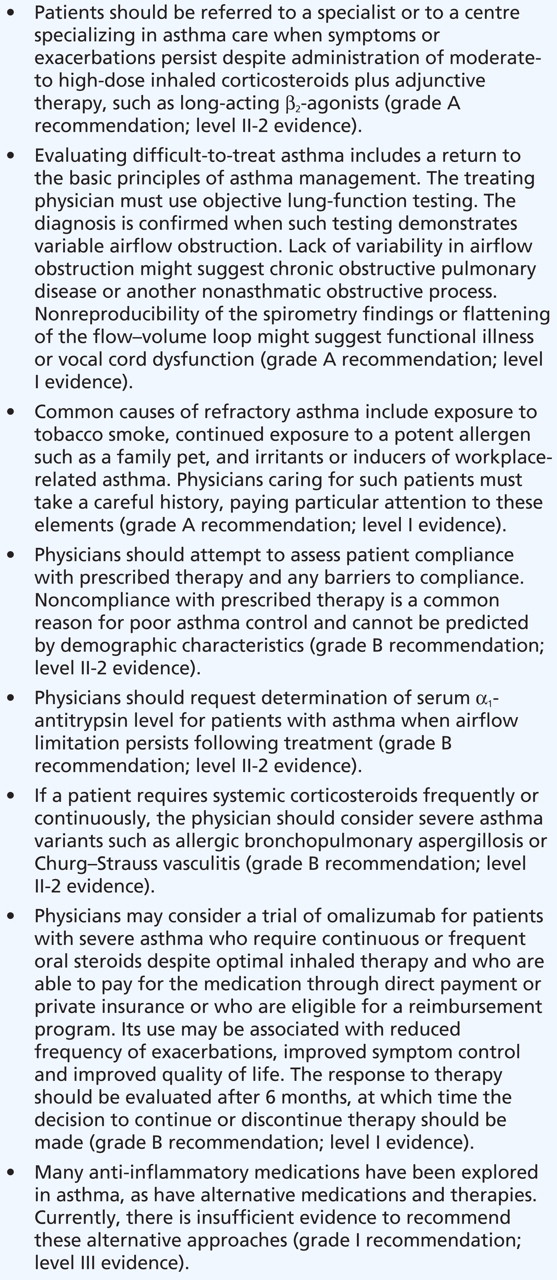
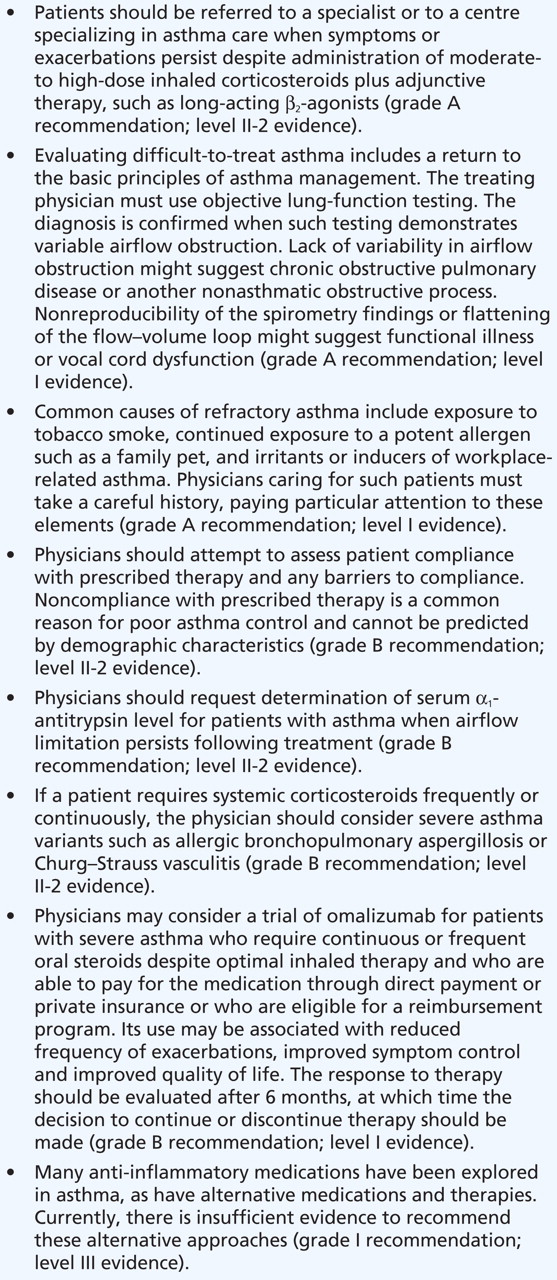
Box 2: Key messages for treatment of asthma unresponsive to usual care
-
The approach to and management of severe asthma is a complex process best implemented in specialized centres.
-
It is crucial to confirm the diagnosis; check inhaler technique and compliance; explore potential triggers, environmental or occupational exposures, and comorbidities; and exclude rare syndromes.
-
Asthma of any severity, particularly if uncontrolled, is associated with increased morbidity and mortality.
-
Therapy in severe asthma must be tailored to the individual patient and monitored regularly.
Key points
Articles to date in this series
-
Subbarao P, Mandhane PJ, Sears MR. Asthma: epidemiology, etiology and risk factors. CMAJ www.cmaj.ca/cgi/doi/10.1503/cmaj.080612
-
Kaplan A, Balter M, Bell A, et al. Diagnosis of asthma in adults. CMAJ www.cmaj.ca/cgi/doi/10.1503/cmaj.080006
-
Balter MS, Bell AD, Kaplan AG, et al. Management of asthma in adults. CMAJ www.cmaj.ca/cgi/doi/10.1503/cmaj.080007
Footnotes
-
Correspondence to: Dr. Kenneth R. Chapman, Asthma and Airway Centre, University Health Network, Toronto Western Hospital, Rm. 7–451 East Wing, 399 Bathurst St., Toronto ON M5T 2S8; kchapman{at}ca.inter.net
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: Kenneth Chapman has received compensation for consulting with AstraZeneca, Boehringer-Ingelheim, CSL Behring, GlaxoSmith-Kline, Merck Frosst, Novartis, Nycomed, Pfizer, Roche, Schering Plough and Talecris. He has undertaken research funded by AstraZeneca, Boehringer-Ingelheim, CSL Behring, Forest Labs, GlaxoSmithKline, Novartis, Parangenix, Roche and Talecris. He has participated in continuing medical education activities sponsored in whole or in part by AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Merck Frosst, Novartis, Nycomed, Pfizer and Talecris. Andrew McIvor has attended advisory board meetings and provided continuing medical education for which he has received honoraria from pharmaceutical companies involved in asthma management: AstraZeneca, Boehringer-Ingelheim, Graceway, GlaxoSmithKlein, Novartis, Merck Frosst and Pfizer.
Contributors: Both authors contributed to the development, writing and editing of the article, and both approved the final version to be published.
Funding: The Canadian Thoracic Society has received funding to facilitate the knowledge translation activities of the CTS Asthma Committee from AstraZeneca Canada, GlaxoSmithKline Inc., Merck Frosst Canada and Novartis Pharmaceuticals. None of the sponsors played a role in the collection, review, analysis or interpretation of the scientific literature or in any decisions regarding the key messages presented in the case studies.
This article is the fourth in a 7-part case study series that was developed as a knowledge translation initiative of the Canadian Thoracic Society Asthma Committee. The series aims to educate and inform primary care providers and nonrespiratory specialists about the diagnosis and management of asthma. The key messages presented in the cases are not clinical practice guidelines but are based on a review of the most recent scientific evidence available. Financial support for the publication of this series has been provided, in part, by the Canadian Thoracic Society.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.
- 48.
- 49.
- 50.↵
- 51.
- 52.
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.
- 71.↵
- 72.↵
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
- Article
- The case
- Sources of information
- Asthma control, severity and unresponsiveness
- Confirming the diagnosis
- Addressing nonpharmacologic aspects of care
- Managing comorbid conditions
- Screening for asthma-associated syndromes
- Monoclonal anti-immunoglobulin E therapy
- Other therapies for severe asthma unresponsive to usual care
- Conclusions
- Articles to date in this series
- Footnotes
- REFERENCES
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

