


- © 2008 Canadian Medical Association
Abstract
Background: Postdischarge use of evidence-based drug therapies has been proposed as a measure of quality of care for myocardial infarction patients. We examined trends in the use of evidence-based drug therapies after discharge among elderly patients with myocardial infarction.
Methods: We performed a cross-sectional study in a retrospective population-based cohort that was created using linked administrative databases. We included patients aged 65 years and older who were discharged from hospital with a diagnosis of myocardial infarction between Apr. 1, 1992, and Mar. 31, 2005. We determined the annual percentage of patients who filled a prescription for statins, β-blockers and angiotensin-modifying drugs within 90 days after discharge.
Results: The percentage of patients who filled a prescription for a β-blocker increased from 42.6% in 1992 to 78.1% in 2005. The percentage of patients who filled a prescription for an angiotensin-modifying drug increased from 42.0% in 1992 to 78.4% in 2005. The percentage of patients who filled a prescription for a statin increased from 4.2% in 1992 to 79.2% in 2005. In 2005, about half of the hospitals had rates of use for each of these therapies that were less than 80%. The temporal rate of increase in statin use after discharge was slower among noncardiologists than among cardiologists (3.5%–2.8% slower). The rate of increase was 4.8% slower for among physicians with low volumes of myocardial infarction patients than among those with high volumes of such patients and was 5.7% greater at teaching hospitals compared with nonteaching hospitals.
Interpretation: Use of statins, β-blockers and angiotensin-modifying drugs increased from 1992 to 2005. The rate of increase in the use of these medications after discharge varied across physician and hospital characteristics.
Pharmacologic therapy is a mainstay in the secondary prevention of coronary artery disease. Acetylsalicylic acid (ASA), β-blockers, angiotensin-converting-enzyme (ACE) inhibitors and statins have all been shown to reduce death and reinfarction among patients who have experienced an acute myocardial infarction. Although these medications have been proven effective in reducing mortality among patients with coronary artery disease, the magnitude of the reduction varies across the different medication classes. Meta-analyses have found that, to avoid 1 death, 83 patients need to receive ASA for a mean duration of 27 months,1 and 42 patients need to receive β-blockers for 2 years.2 In comparison, to avoid 1 death among patients with heart failure or left ventricular dysfunction, 15 patients need to receive ACE inhibitors for 2.5 years.3 Finally, 61 patients need to receive statins for a mean duration of 5.4 years to avoid 1 death.4
Between the late 1980s and mid-1990s, several studies documented the underuse of evidence-based pharmacologic therapies among patients with myocardial infarction.5–12 Less is known about the recent trends in the use of these therapies. We examined the trends in the use of evidence-based drug therapies after discharge in a population-based sample of elderly patients diagnosed with myocardial infarction. We also sought to identify physician and hospital characteristics associated with a more rapid temporal increase in the use of these therapies.
Methods
Study design and population
We performed a cross-sectional study with a retrospective population-based cohort. We used data from the Ontario Myocardial Infarction Database, a population-based database of patients admitted to hospital with myocardial infarction in Ontario between Apr. 1, 1992, and Mar. 31, 2005. This database was created by linking together data from several health care administrative databases. Its creation is described in greater detail elsewhere.13,14 This database contains data from the Ontario Drug Benefit database, which tracks the use of prescription medications by all Ontario residents aged 65 years and older. Therefore, our study was restricted to patients aged 65 years and older who were discharged from hospital with a diagnosis of myocardial infarction. Patients who had been admitted to hospital with myocardial infarction in the year before the index admission were excluded to restrict the sample to patients with new diagnoses. We also excluded patients discharged to complex continuing care hospitals because their medications are not covered under the Ontario Drug Benefit program. The accuracy of the most responsible diagnosis of myocardial infarction upon which patients were selected for inclusion has previously been validated. It was shown to have a specificity of 92.8% and a sensitivity of 88.8% among patients admitted to coronary care units.15
Medication use
We compared patients' demographic and clinical characteristics across different periods of the study. For each year, we determined the percentage of patients aged 65 and older who, within 90 days after discharge from hospital, filled a prescription for each of the following medical therapies: β-blockers, angiotensin-modifying agents (either ACE inhibitors or angiotensin-receptor blockers) and statins. The reasons for using a 90-day window and for combining ACE inhibitors and angiotensin-receptor blockers are described in an online appendix (available at www.cmaj.ca/cgi/content/full/179/9/895/DC2). We did not examine postdischarge use of ASA because it is available without a prescription; thus, its use is not accurately captured by the Ontario Drug Benefit program.
Physician and hospital characteristics
We conducted a second set of analyses to determine the physician and hospital characteristics that were associated with a more rapid temporal increase in the postdischarge use of evidence-based medications. We included physician specialty and sex as well as the average annual volume of patients with myocardial infarction seen (all ages) and the average number of years of clinical experience across the study period. Only years in which the physician saw at least 1 patient with myocardial infarction were used to calculate the average annual volume. We included the following hospital characteristics: teaching status and average annual volume of patients with myocardial infarction (all ages) during the study period.
Statistical analysis
We compared patients' demographic and clinical characteristics across different periods of the study. Categorical variables were compared using the χ2 test, and continuous variables were compared using the Wilcoxon rank-sum test. We assessed the statistical significance of the trends in medication prescribing using the Mantel–Haenszel χ2 test.
We used random-effects logistic regression models to examine the influence of patient, physician and hospital characteristics on postdischarge medication use.16 The models included the following patient-level variables: age, sex and the 9 comorbid conditions (cardiogenic shock, congestive heart failure, pulmonary edema, cardiac dysrhythmia, malignant disease, cerebrovascular disease, acute renal failure, chronic renal failure, diabetes with complications) that comprise the Ontario acute myocardial infarction mortality prediction model. The derivation and validation of this model has been described elsewhere.17 The regression models incorporated a variable denoting the number of years since 1992, which allowed us to determine changes in the use of each medical therapy over time. We modified each model by incorporating an interaction between time and each physician and hospital characteristic. This allowed us to examine whether the rate of increase in the use of medical therapies differed depending on physician or hospital characteristics. Because of the size and complex nature of the sample, a cross-classified multilevel was not fit. As was done in an earlier study, if physicians practised at 2 different hospitals, we considered them to be 2 independent physicians.18
Results
Study population
During the study period, 132 778 elderly patients with a myocardial infarction were discharged from hospital. The patient demographic and clinical characteristics are reported in Table 1. The median patient age and prevalence of each of the comorbid conditions examined varied across the different periods of the study (p ≤ 0.025). Because of the large sample, judgment should be used in interpreting the clinical significance of differences between the different eras.
Table 1.
Overall trends
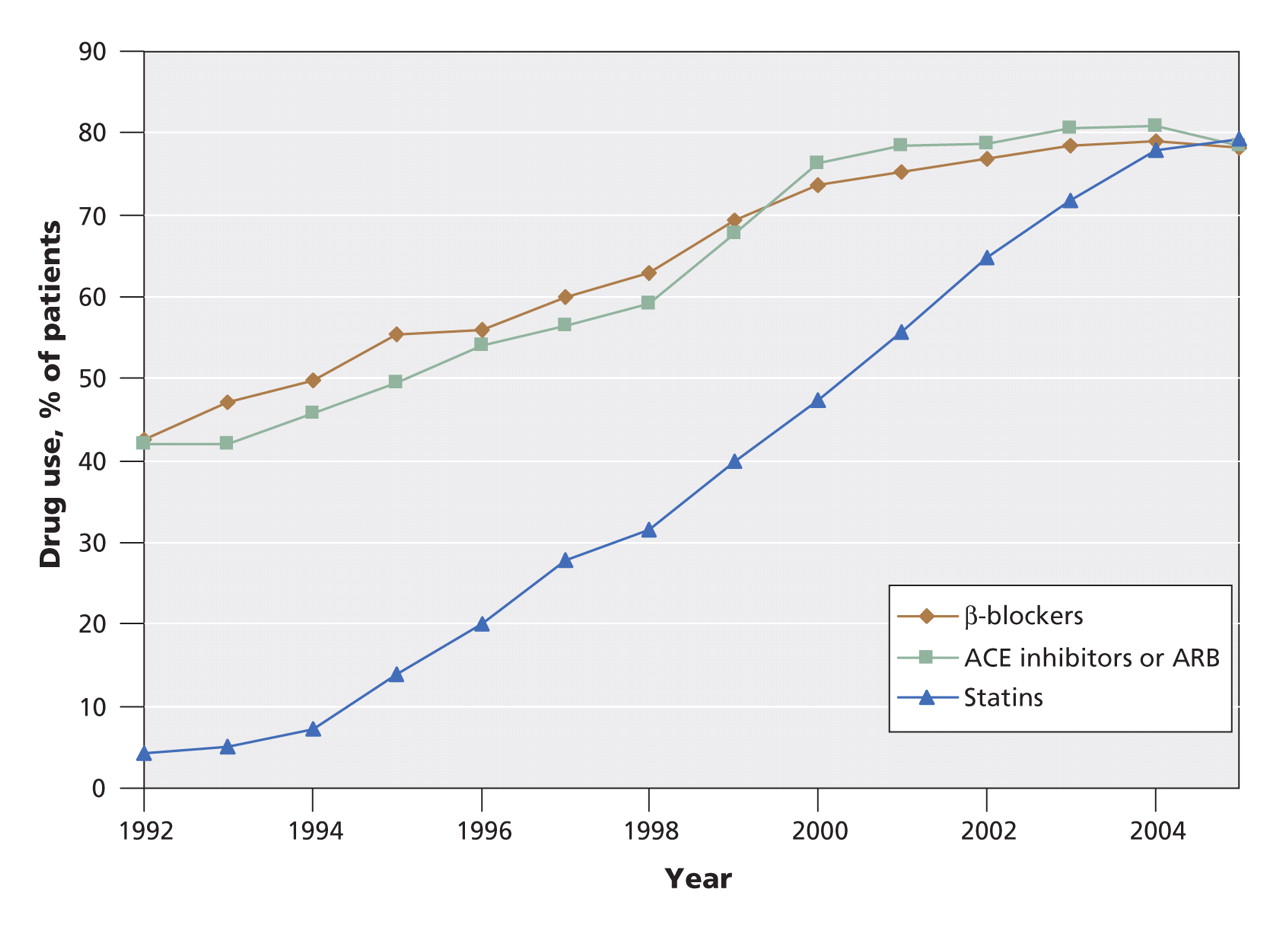
The annual number of elderly patients with myocardial infarction ranged from 8133 in 1992 to 10 707 in 2001. Overall trends in the postdischarge use of evidence-based therapies are described in Figure 1. In 1992, 42.6% of the patients filled a prescription for a β-blocker within 90 days after discharge. This percentage increased to 78.1% in 2005. The percentage of patients who filled a prescription for an angiotensin-modifying agent increased from 42.0% in 1992 to 78.4% in 2005. The percentage of patients who filled a prescription for a statin increased from 4.2% in 1992 to 79.2% in 2005. The increase in the rate of use of each class of medications was statistically significant across the study period (p < 0.001). Postdischarge use of each of the different classes of medications appeared to plateau in either 2002 or 2003. In 2005, prescriptions for β-blockers, angiotensin-modifying agents and statins were filled by about 80% of the patients after discharge. We found similar trends when we examined hospital-specific rates of medication use after discharge. Since 2003, about 50% of the hospitals had rates of β-blocker use that exceeded 80%, and since 2001, about 50% of the hospitals had rates of use of angiotensin-modifying drugs that exceeded 80%. In 2005, over 50% of the hospitals had rates of statin use that exceeded 80%. Conversely, even during the last years of the study, about half of the included hospitals had rates that were less than 80% for each medication.
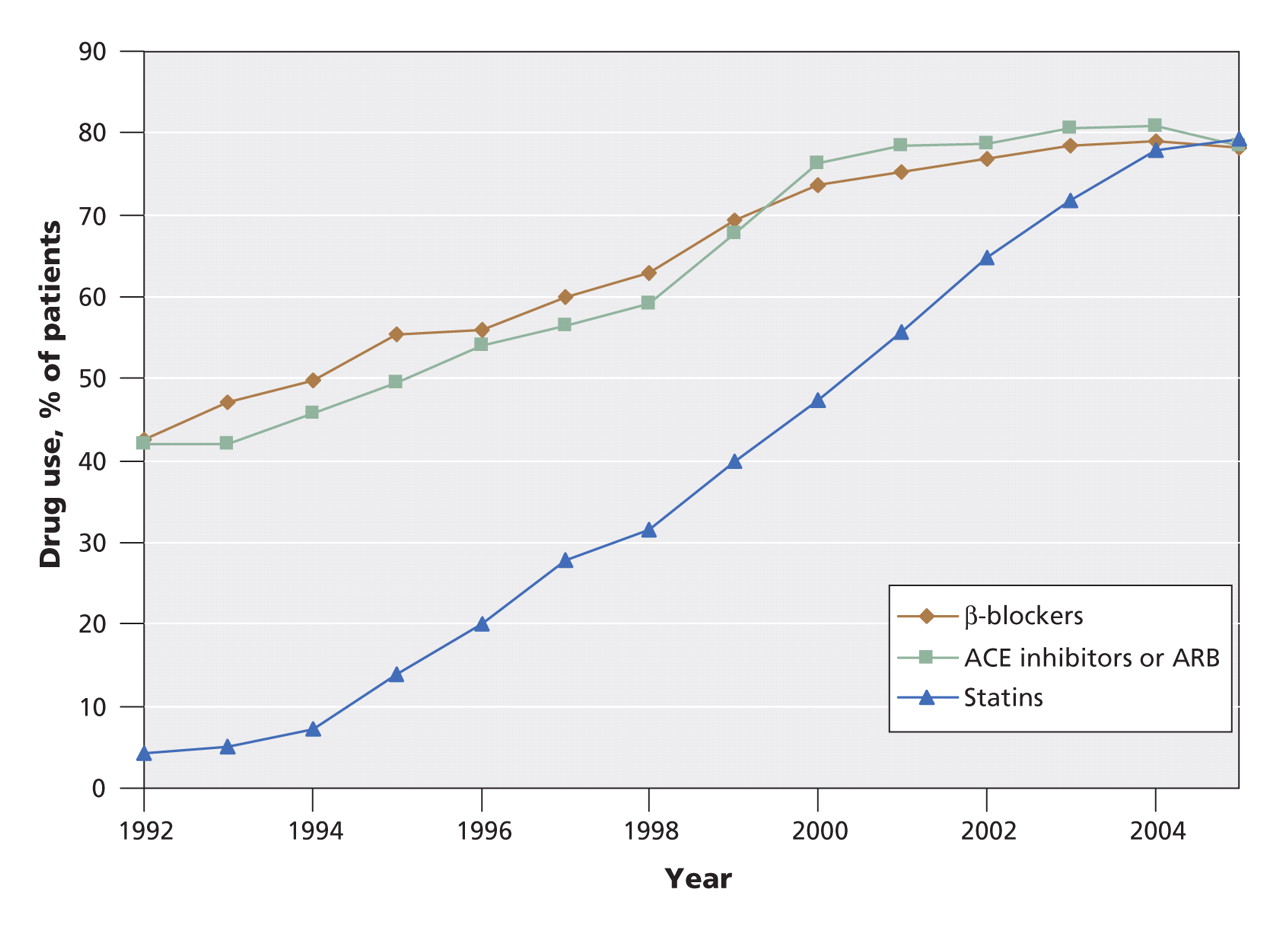
Figure 1: Use of evidence-based drug therapies after discharge among elderly patients with acute myocardial infarction, from 1992 to 2005. Note: ACE = angiotensin-modifying enzyme, ARB = angiotensin-receptor blocker.
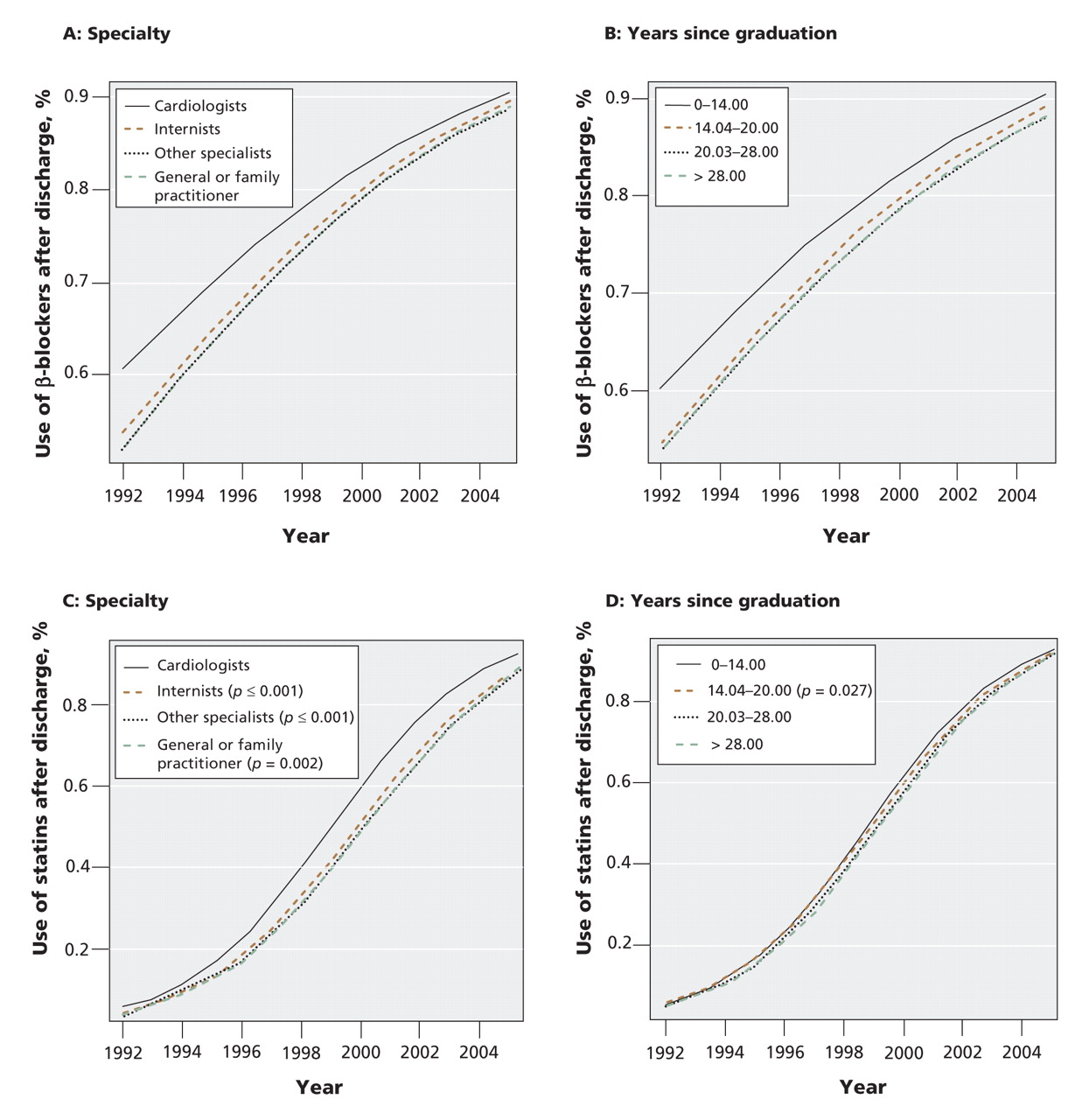
The results of our analyses to examine physician and hospital characteristics associated with a more rapid increase in postdischarge use of β-blockers, angiotensin-modifying agents and statins are described in Figure 2 and Appendix 2 (available online at www.cmaj.ca/cgi/content/full/179/9/895/DC2). For each physician for which the rate of uptake of evidence was different from the reference group, we provide a ratio and associated 95% CI. This ratio describes the relative difference between the odds ratio for the temporal increase in prescribing in the given group and the odds ratio for the temporal increase in prescribing in the reference group.
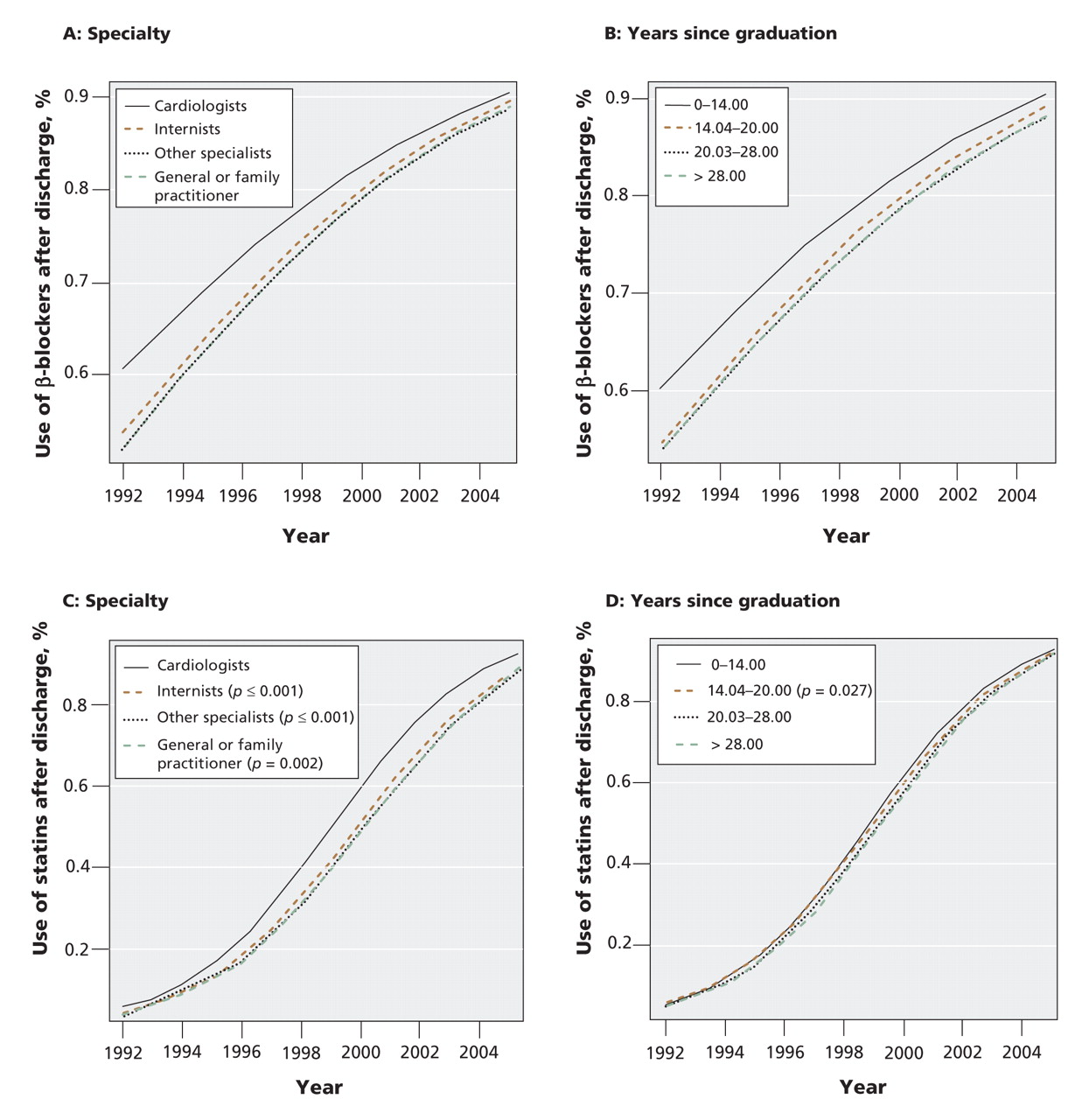
Figure 2: Physician characteristics associated with the temporal rate of increase in the use of β-blockers (A, B) and statins (C, D) from 1992 to 2005. The plotted probabilities of medication use after discharge were derived from the fitted multilevel regression model and represent the predicted probability at an average hospital, for a patient of average age, all of whose risk factors were set to absent, and whose values for the other physician and hospital characteristics were set to their reference levels.
Physician characteristics and postdischarge prescribing
The rate of increase in postdischarge use of β-blockers was greater among general internists (1.02, 95% confidence interval [CI] 1.00–1.03, p = 0.008) and other specialists (1.02, 95% CI 1.00–1.03, p = 0.016) than among cardiologists. The annual increase in the odds of postdischarge β-blocker use was 1.6% greater among general internists than among cardiologists. The rate of increase in postdischarge use of β-blockers was greater among female physicians than among male physicians (1.02, 95% CI 1.01–1.03, p = 0.002). The rate of increase in β-blocker prescribing was slower among physicians in the lowest quartile of annual volume of myocardial infarction patients (0.98, 95% CI 0.97–1.00, p = 0.041) and second lowest (0.99, 95% CI 0.97–1.00, p = 0.047) than among physicians in the highest quartile.
The rate of increase in postdischarge use of angiotensin-modifying agents was slower among internists (0.98, 95% CI 0.97–0.99, p = 0.001) and other subspecialists (0.98, 95% CI 0.97–1.00, p = 0.016) than among cardiologists. The rate of increase was also slower among physicians in the lowest (0.94, 95% CI 0.93–0.96, p < 0.001) and second lowest (0.98, 95% CI 0.97–1.00, p = 0.014) quartiles of annual volume of myocardial infarction patients than among physicians in the highest quartile.
The rate of increase in postdischarge use of statins was slower among general and family practitioners (0.97, 95% CI 0.94–0.99, p = 0.002), general internists (0.97, 95% CI 0.96–0.99, p < 0.001) and other specialists (0.97, 95% CI 0.95–0.99, p < 0.001) than among cardiologists. The rate of increase was slower among physicians in the lowest quartile of annual volume of myocardial infarction patients than among physicians in the highest quartile (0.95, 95% CI 0.93–0.97, p < 0.001). The rate of increase was also slower among physicians with 14.04–20.00 years of clinical experience than among those with less experience (0.98, 95% CI 0.97–1.00, p = 0.027).
Hospital characteristics and postdischarge prescribing
Postdischarge use of β-blockers increased less rapidly at teaching hospitals than at nonteaching hospitals (0.98, 95% CI 0.97–0.99, p < 0.001). The rate of increase in statin use was greater at teaching hospitals than at nonteaching hospitals (1.06, 95% CI 1.04–1.07, p < 0.001).
Interpretation
We observed gradual and substantial increases between 1992 and 2005 in the postdischarge use of β-blockers, angiotensin-modifying agents and statins among elderly patients with myocardial infarction. The use of β-blockers and angiotensin-modifying agents approximately doubled over the study period, and the use of statins increased 18-fold. Furthermore, at the population level, the use of each of these therapies appears to have reached a plateau.
A novel contribution of our study is that it examined the association of physician and hospital characteristics with temporal changes in the use of evidence-based drug therapies. Although we did not find a consistent pattern across the 3 classes of medications, we found an association between physician and hospital characteristics and the rate of increase in the postdischarge use of each of the 3 medication classes over time. For example, in 1992 β-blocker use was higher among patients attended by cardiologists than among those attended by noncardiologists. However, the rate of increase in the prescribing of β-blockers was greater among general internists and other specialists than among cardiologists, such that postdischarge rates were converging between the different specialties by the end of the study period.
The temporal increase in postdischarge statin use was greater among patients attended by cardiologists than among those attended by noncardiologists. An explanation for this difference may be the temporality of the availability of evidence. Evidence for statin use in myocardial infarction patients accumulated in the 1990s, which comprised the early part of our study period. In contrast, evidence for β-blocker use in this population accumulated in the 1980s, before our study period. Thus, cardiologists may have been aware of the evidence for β-blockers, while it took longer for this evidence to disseminate among noncardiologists. Finally, the temporal rate of increase in postdischarge use of angiotensin-modifying agents was greater among cardiologists than among internists and other specialists. Evidence for the use of angiotensin-modifying agents accumulated during the study period, and cardiologists may have had a better awareness of this evidence.
The overall trends in our study are similar to those of a recent study that examined the trends in quality of care provided to myocardial infarction patients in 4 US states between 1992 and 2001.19 That study found improvements, among all patients and ideal candidates, in prescribing at discharge of ASA, β-blockers and ACE inhibitors between 1992 and 2001. Importantly, only a minority of patients were identified as ideal candidates for each therapy. In 2000/01, among all patients, the discharge rates of prescribing ASA, β-blockers and angiotensin-converting enzyme inhibitors were 79.4%, 71.4% and 64.6%, respectively. Among ideal candidates, prescribing rates were 87.4%, 80.3% and 74.8%, respectively.
Our findings are also relevant to policy-makers and clinicians interested in quality improvement for cardiac care. The steady, as opposed to abrupt, increase in the rates of use of drug therapies for the secondary prevention of myocardial infarction over our 14-year study period suggests that changing physician prescribing behaviour is a process that happens slowly over time and that it is achievable with sustained reinforcement. Multiple clinical trials and observational studies that expanded the indications and documented the underuse of these therapies were published during the study period. Our results suggest that these studies likely had a cumulative effect that eventually resulted in close to saturation levels of therapy for secondary prevention.
When restricted to agents for which evidence was disseminated during the study period (angiotensin-modifying agents and statins), our study provides some evidence that cardiologists adapt evidence-based medication use more rapidly than noncardiologists. Furthermore, physicians who cared for a low number of patients with myocardial infarction tended to adopt evidence-based care more slowly than those who cared for many such patients. Finally, teaching hospitals adopted the use of statins more rapidly than nonteaching hospitals. Our findings suggest that there is a need to identify methods to stimulate more rapid uptake of evidence-based drug therapies by physicians practising in nonteaching hospitals, as well as by noncardiologists and physicians who care for a low number of patients with myocardial infarction. Providing low-volume physicians with mentors and encouraging academic institutions to partner with nonteaching hospitals may result in a more rapid uptake of evidence. Finally, we speculate that the development and rapid dissemination of standardized discharge checklists by cardiovascular specialists could improve the uptake of evidence-based practices by groups in which uptake has been historically slower.
Bradley and colleagues conducted a qualitative study to identify factors associated with an increase in β-blocker use after myocardial infarction.20 They found that hospitals with greater temporal improvements in β-blocker use had 4 characteristics not found in hospitals with less or no temporal improvement: shared goals for improvement, substantial administrative support, strong physician leadership advocating β-blocker use and use of credible data feedback.20 The final element suggests that hospital report cards that include hospital-specific postdischarge rates of medication use among myocardial infarction patients, similar to one published earlier in Ontario,21 may help to improve evidence-based prescribing.
Limitations
There are limitations to our study. First, we used administrative data, which did not allow us to exclude patients who had contraindications to the therapies under consideration. However, as found elsewhere,19 it is likely that postdischarge medication use is even higher among ideal patients for whom therapy is indicated and who have no contraindications than it is in the entire population of patients with myocardial infarction. Furthermore, our use of administrative data allowed us to examine use of prescription medications by all elderly patients with myocardial infarction in our jurisdiction. The data for our study were from a population-based database of incident hospital admissions of patients with myocardial infarction in Ontario. Therefore, our data are comprehensive and not restricted to only tertiary centres or to a registry that is subject to voluntary enrolment.
A second limitation is that we reported the percentage of patients who filled a prescription. We were unable to capture prescriptions that were not filled by the patient. Therefore, our results likely underestimate postdischarge prescribing.
A third limitation is that our analyses were restricted to patients aged 65 and older. Earlier studies have shown that prescribing of evidence-based therapies after myocardial infarction decreases with increasing age.6,7,11 Thus, the use of these therapies is likely even higher among younger patients.
Conclusion
Prescriptions for β-blockers, angiotensin-modifying agents and statins are currently filled by about 80% of elderly patients with myocardial infarction after discharge from hospital. However, there was moderate variation in hospital-specific rates of use of these therapies, with about half of all hospitals prescribing these medications to less than 80% of patients. Furthermore, the rate of increase in use of evidence-based drug therapies use depended on physician and hospital characteristics.
@@ See related research, page 901, related commentary, page 875, and related review, page 909
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/179/9/895/DC1
Funding: This research was supported by an operating grant from the Heart and Stroke Foundation of Ontario and a Canadian Institutes of Health Research Team Grant in Cardiovascular Outcomes Research.
This article has been peer reviewed.
Contributors: Peter Austin and Jack Tu contributed substantially to the conception and design of the article. All of the authors contributed to the interpretation of data. Peter Austin drafted the article; Dennis Ko, David Alter and Jack Tu revised the manuscript critically for important intellectual content. All of the authors approved the version submitted for publication. Peter Austin had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyses.
Acknowledgements: The Institute for Clinical Evaluative Sciences is supported in part by a grant from the Ontario Ministry of Health and Long-Term Care. The opinions, results and conclusions are those of the authors, and no endorsement by the Ontario Ministry of Health and Long-Term Care or by the Institute for Clinical Evaluative Sciences is intended or should be inferred.
Peter Austin is supported in part by a Career Scientist Award from the Heart and Stroke Foundation of Ontario. Dennis Ko is supported by a Clinician–Scientist Award by the Heart and Stroke Foundation of Ontario. Jack Tu holds a Canada Research Chair in Health Services Research and a Career Investigator Award from the Heart and Stroke Foundation of Ontario.
Competing interests: David Alter is the chief scientific officer of INTERxVENT Canada. No competing interests declared by Peter Austin, Jack Tu or Dennis Ko.
REFERENCES
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- In-hospital myocardial infarction and adherence to evidence-based drug therapies: a real-world evaluation
- Relationship Between Care Gaps and Projected Life Expectancy After Acute Myocardial Infarction
- Trends in 1-year survival of people admitted to hospital in Ontario, 1994-2009
- Myocardial infarction and quality of care
- Factors associated with the use of evidence-based therapies after discharge among elderly patients with myocardial infarction
More in this TOC Section
Similar Articles

