


- © 2007 Canadian Medical Association or its licensors
What's your call?
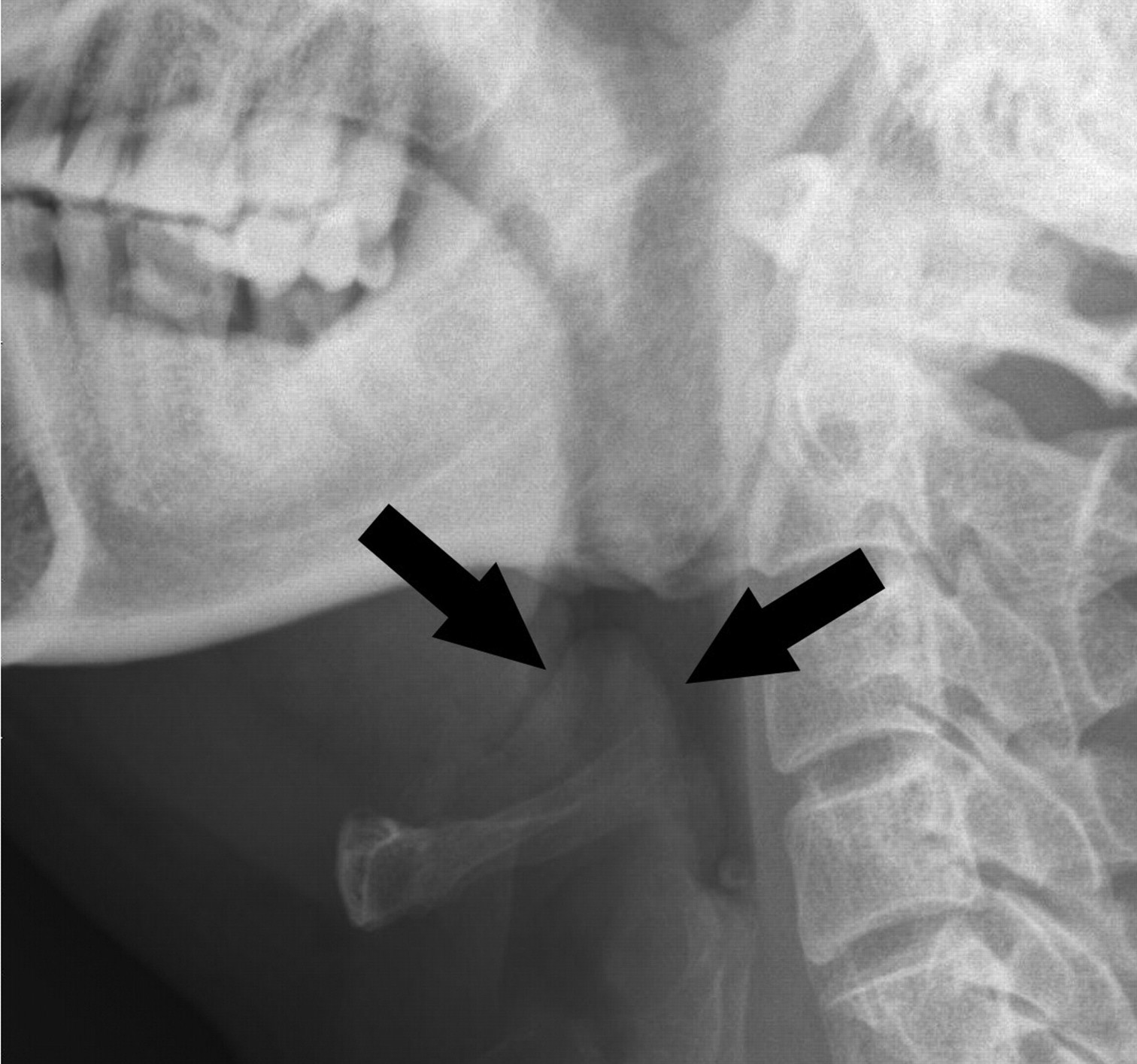
Figure. Soft-tissue radiograph of the neck of a 46-year-old man who presented to the emergency department with a 3-day history of fever, sore throat, dysphagia, odynophagia, drooling and a muffled voice.
The radiograph showed the classic “thumbprint sign” (Fig. 1, arrows) characteristic of epiglottitis. The patient had progressive respiratory distress and required emergent endotracheal intubation. A swollen epiglottis was seen under direct laryngoscopy. It almost obstructed the airway and allowed only a small-caliber endotracheal tube to pass through. Parenteral therapy with amoxicillin–clavulanate and corticosteroids was begun. The patient recovered well, and the endotracheal tube was removed on day 5, after resolution of the swelling was confirmed with flexible laryngoscopy.
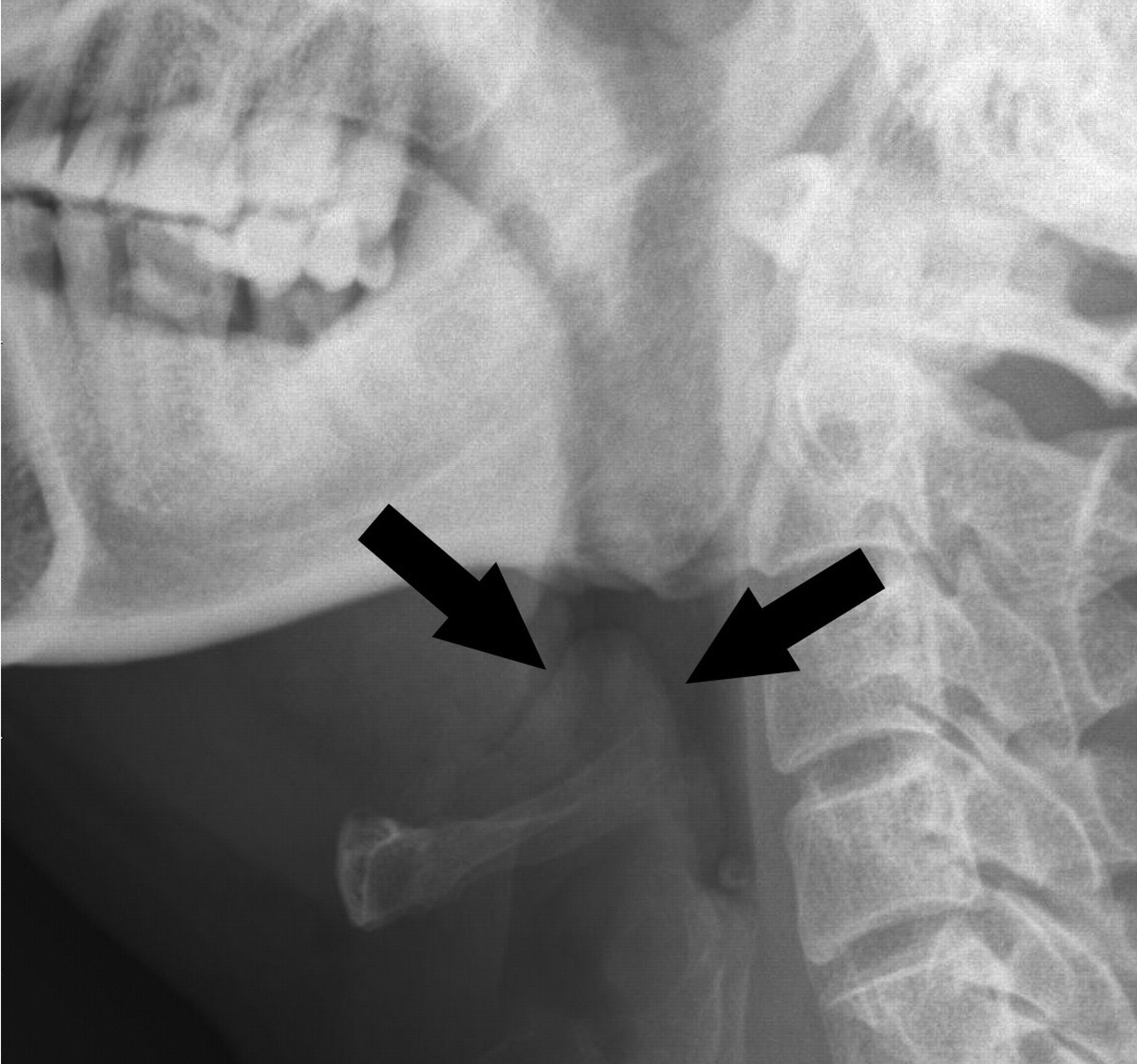
Fig. 1: Classic “thumbprint sign” (arrows) characteristic of epiglottitis.
Before the widespread use of the Haemophilus influenzae type b vaccine, epiglottitis occurred mainly in young children. Recently, the incidence has decreased among children and increased among adults.1 Adult epiglottitis is different from its pediatric counterpart in that organism identification is less common2 and the mortality is higher. From 15% to 21% of patients require either endotracheal intubation or emergent tracheostomy.1,3 The remaining cases can be safely treated with antibiotics. In certain cases intravenous corticosteroid therapy may be of benefit.
The most common symptoms are sore throat, odynophagia and muffled voice.3 Soft-tissue lateral neck radiography has a sensitivity of 88%, whereas laryngoscopy is the most accurate investigation to establish a diagnosis.2 Prompt recognition of the condition and early airway intervention in cases of airway compromise are crucial to avoid a possible fatal outcome.
Footnotes
-
Competing interests: None declared.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

