


- © 2007 Canadian Medical Association or its licensors
A healthy, 39-year-old man who works at construction sites arrived with a 1-year history of “electric shocks” in his right foot whenever he wore his work boots. This was initially attributed to ill-fitting footwear. In time, his symptoms persisted even after removing his boots, and he noted a small nodule on the inside of his right ankle. The patient could not recall any instance of injury to his right foot before the swelling developed. Mild pressure on this spot worsened his discomfort.
In view of his worsening symptoms, the development of a swelling and failures of nonsurgical treatments (e.g., better-fitting boots, splinting), the patient was referred to the neurosurgical team. He was found to have reduced pinprick sensation in the anterior half of his right sole, the balls of all those toes and the middle of his right heel (Fig. 1). The small cystic swelling, which moved when the big toe was flexed, was located just below his medial malleolus. Tapping over the swelling caused paresthesia in the middle 3 toes and medial sole of his right foot.
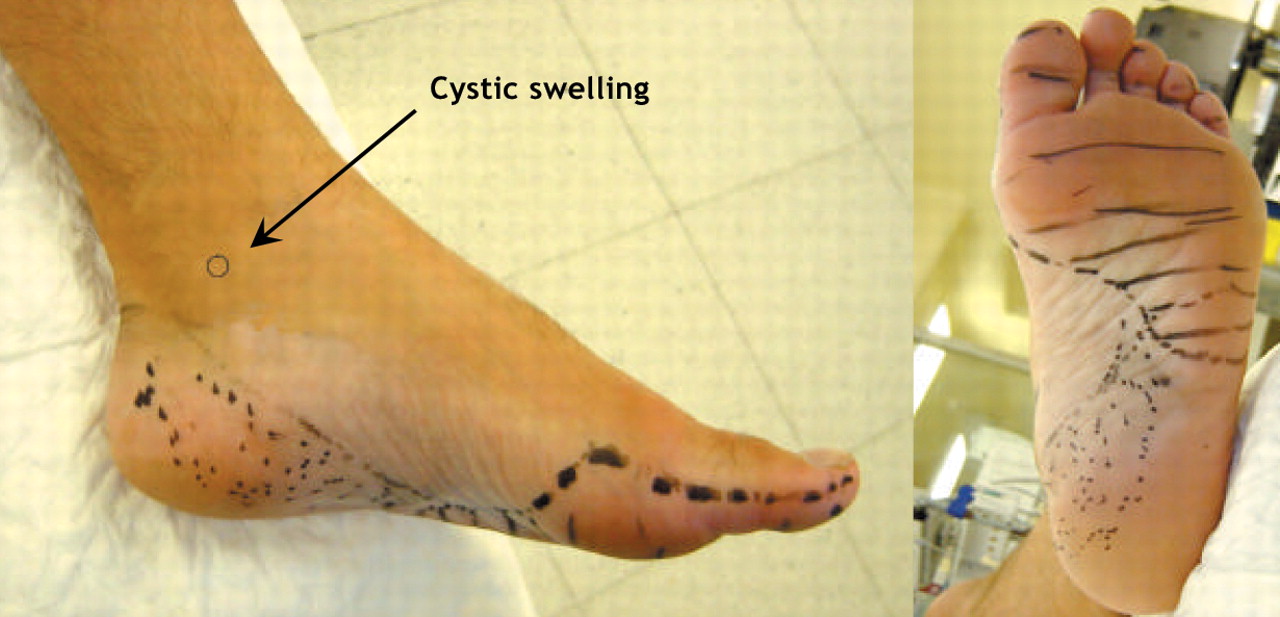
Fig. 1: The patient's foot, showing the regions of reduced sensation found with the pinprick test: striped, for the area served by the cutaneous branches of the plantar nerve; and dotted, the medial calcaneal nerve.
The foot was not deformed, and ankle movements were full and pain-free. Moderate direct pressure on the sole failed to recreate his symptoms. There was possibly some weakness of the right abductor hallucis muscle but no muscle wasting in the right foot, nor any weakness in toe or ankle flexion or extension. The dorsum of the right foot showed normal sensation.
The area of the sensory disturbances conformed to the cutaneous territory of the medial calcaneal and the medial and lateral plantar branches of the posterior tibial nerve. A diagnosis of tarsal tunnel syndrome was made, and confirmed neurophysiologically.
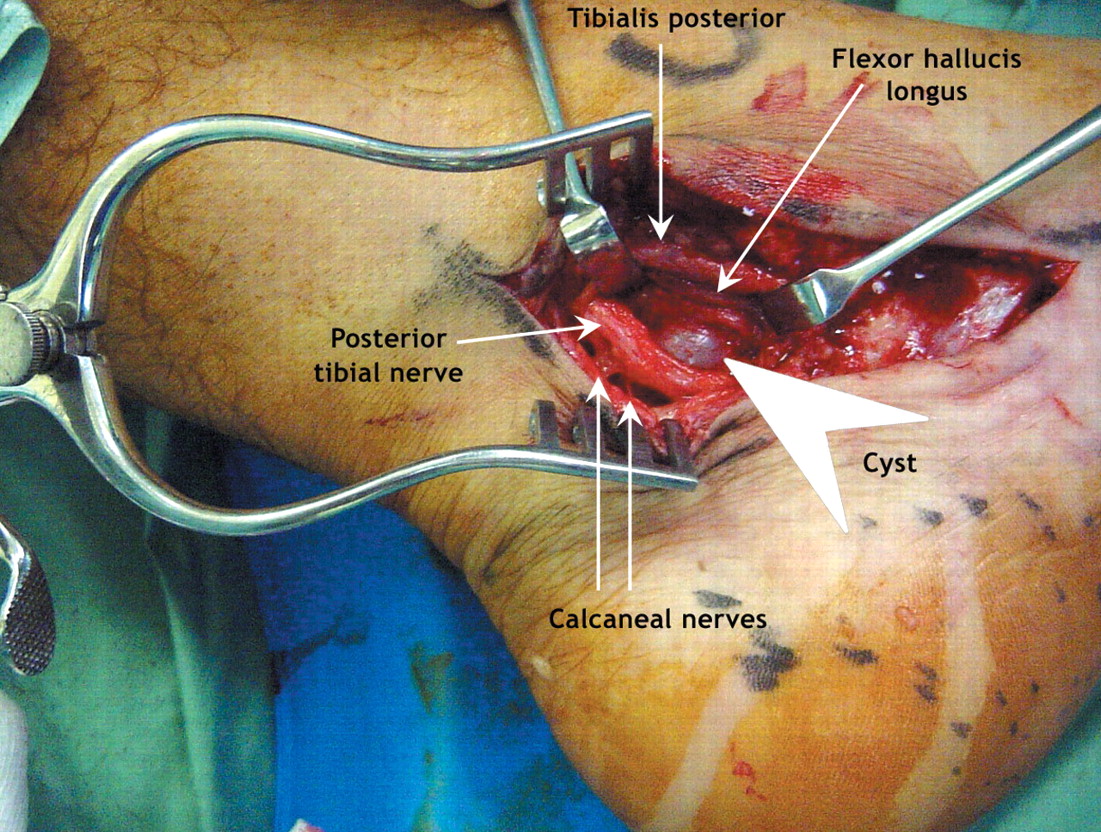
When the tarsal tunnel was explored surgically, the calcaneal and plantar nerves were found to be compressed by a ganglion arising from the sheath of the flexor hallucis longus tendon (Fig. 2). The cyst was completely excised; the patient's symptoms resolved, with no recurrence as of 2 years of follow-up. Histological examination of the excised tissue confirmed the surgical diagnosis of a ganglion cyst.
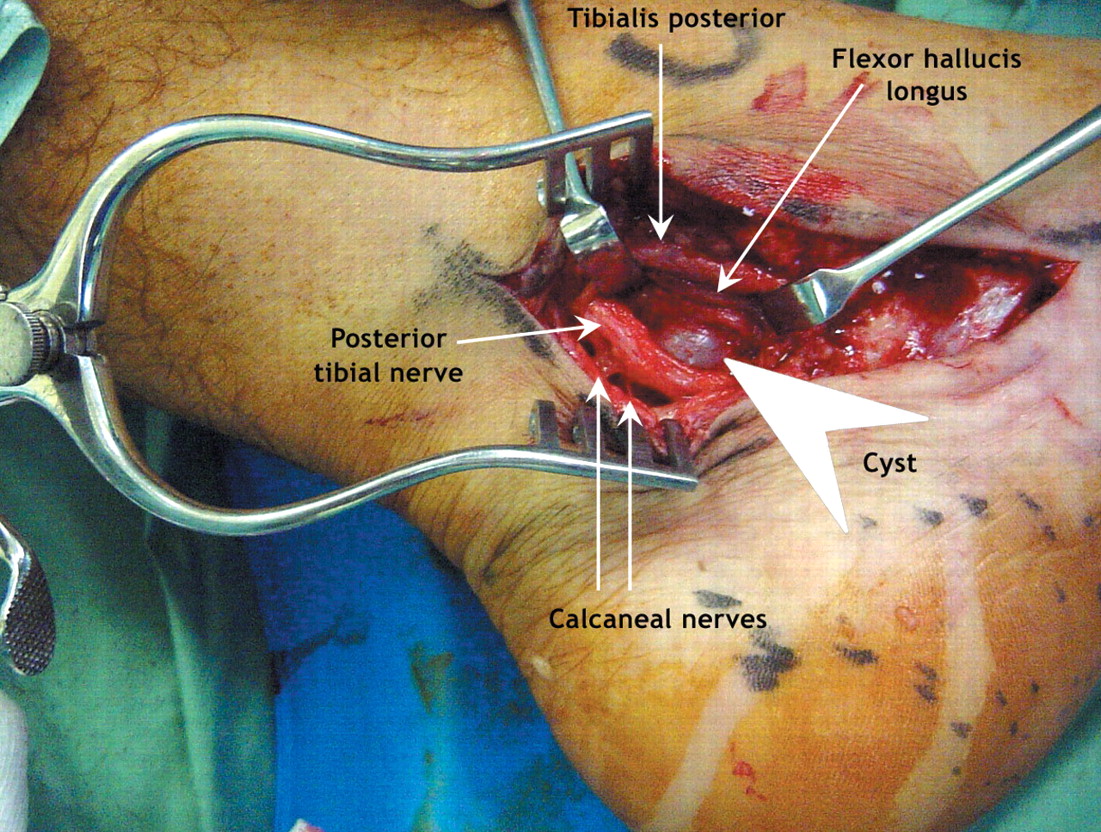
Fig. 2: Surgery to remove the ganglion (arrowhead) found to be compressing the patient's calcaneal and medial plantar nerves.
The tarsal tunnel is a fibro-osseous tunnel through which the distal posterior tibial nerve and its branches (the calcaneal nerve and the medial and lateral plantar nerves) pass as they curve around the medial malleolus into the foot. Entrapment of these nerves at this point results in the tarsal tunnel syndrome. The symptoms may vary according to the nerves affected:1 the calcaneal nerves are purely sensory and supply the heel; the medial plantar nerve innervates the medial aspect of the sole and the medial 3 or 4 toes and their associated muscles; and the lateral plantar nerve supplies the remainder of the skin on the plantar aspect of the sole and toes, and the small muscles that control the lateral toes. The muscles responsible for ankle movements are unaffected.
Tarsal tunnel syndrome is an uncommon entrapment neuropathy caused by several conditions, of which ganglion cysts are one. Most ganglion-associated neuropathy involves the peroneal nerve;2 cysts involving the posterior tibial nerve account for only 4% of cases.2 Despite debate about the actual causes of these cysts, most believe that they usually arise from joint capsules or tendon sheaths.2 Local trauma or stresses appear to play an important role.3 In this case, we hypothesize that repeated local microtrauma from the wearing of boots caused a ganglion cyst to form from the sheath of the flexor hallucis longus tendon.
Outcomes after surgical removal of ganglion cysts that cause entrapment neuropathies are usually good,1–3 although a 17% recurrence of symptoms during long-term follow-up despite complete surgical resection has been reported.2
Although tarsal tunnel syndrome is an uncommon clinical entity, it should always be considered during the differential diagnosis of foot pain, especially if clinical features conform to the distribution of the posterior tibial nerve and its branches.
Footnotes
-
Competing interests: None declared.
In this issue
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

