


Pertussis remains one of the least well-controlled vaccine-preventable diseases for which routine vaccination exists. Although most often a persistent but relatively benign respiratory illness, pertussis can result in serious consequences, such as pneumonia, seizures, encephalopathy and death, especially among infants.
Pertussis whole-cell vaccine was introduced in Canada in 1943, and the reported incidence of the disease dropped by 90% in the ensuing 40 years. However, it increased again in the early 1990s and has remained high since then (Fig. 1). A 5-component acellular pertussis vaccine became available in 1997. This vaccine has a lower incidence of adverse reactions and a higher efficacy (3 doses prevented 85% of cases over a 2-year period)1 than the whole-cell vaccine used in Canada (efficacy of less than 60% for 5 doses).2 Pertussis vaccine coverage rates remained stable in Canada between 1985 and 2002: during that period 80%–91% of children received 3 doses by age 2.3

Fig. 1: Pertussis incidence rate, Canada, 1924–2002. The incidence dropped after a vaccine was introduced in 1943 and reached an all-time low of 4.3 per 100 000 in 1988. Since then, the incidence has increased again, remaining between 9.5 and 35 per 100 000 per year between 1991 and 2002, with an average of 5720 cases reported each year.
Pertussis is most easily diagnosed in young children because they present with whooping cough, which is characterized by paroxysmal coughing followed by an audible inspiratory whoop and, occasionally, vomiting. Infants, immunized children, adolescents and adults do not usually exhibit whooping cough. Infants often present with cough and apneic episodes. They can be severely ill and may require admission to hospital. Adolescents and adults may be asymptomatic or present with a cough lasting several weeks. Although pertussis is a reportable disease, recognition of the illness by physicians is hampered by the nonspecific symptoms in adolescents and adults.
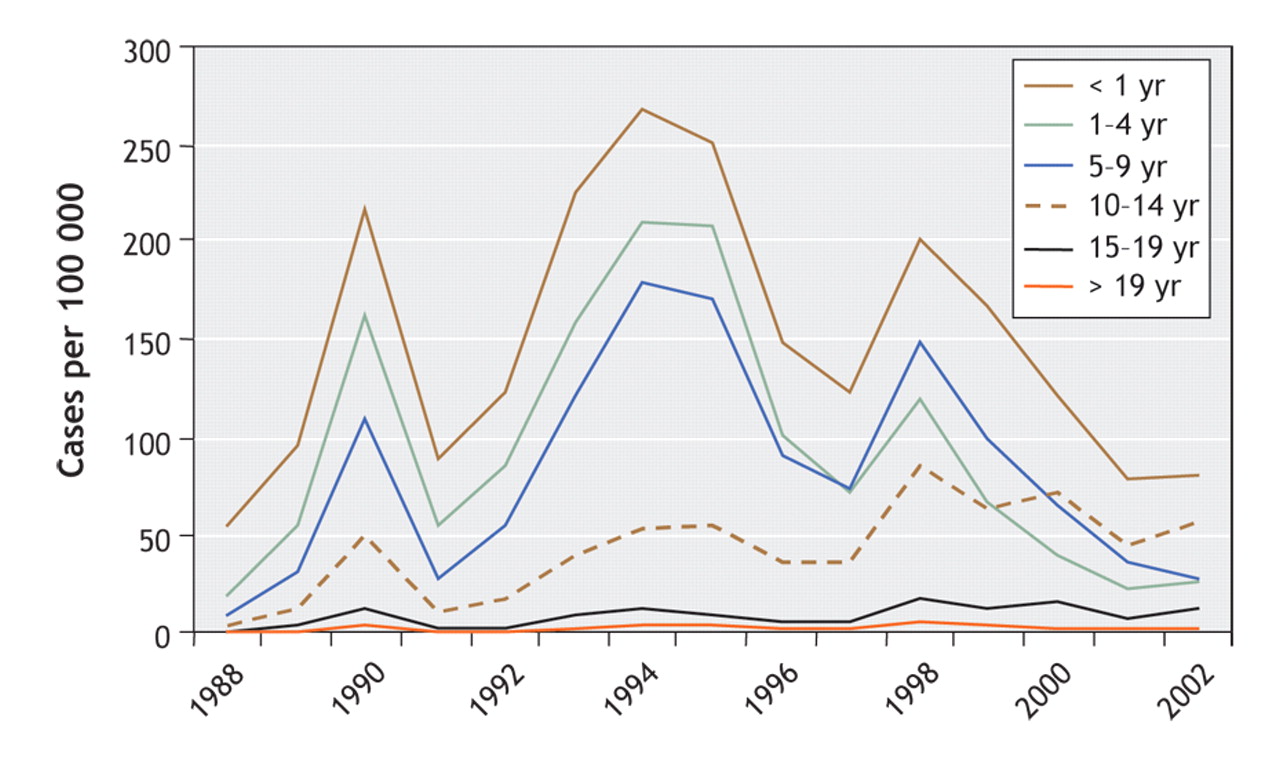
Interpreting changes in pertussis incidence rates is challenging. An increased awareness among physicians of the clinical presentation of the disease in adolescents and adults may explain some of the increase in reported cases in these age groups in the 1990s (Fig. 2). Pertussis can be diagnosed by culture and polymerase chain reaction testing of a nasopharyngeal swab or aspirate. Polymerase chain reaction testing became widely available in Canadian hospitals and laboratories in the mid-to late 1990s, which increased the capacity to diagnose the disease.

Fig. 2: Age-specific pertussis incidence rates, Canada, 1988–2002. The highest incidence has remained among infants. The incidence has been dropping among children younger than 10 years of age since 1998, but in the 1990s it increased among those 10 years and older. Since 2000, children 10–14 years of age have had the second highest incidence after that observed among infants. The proportion of cases among adults (> 19 years) increased from 6% of all cases in 1988 to 18% of all cases in 2002.
However, most of the recent increase in the rate of pertussis is due to waning natural and vaccine-induced immunity, which occurs 6–12 years after the last episode of illness or booster dose. The highest increase in rates of the disease in the 1990s was among adolescents and adults. During this decade, excluding infants, the highest incidence was observed in a cohort of children born between 1988 and 1992 (Fig. 3) who received a low-efficacy whole-cell vaccine and experienced early waning immunity.
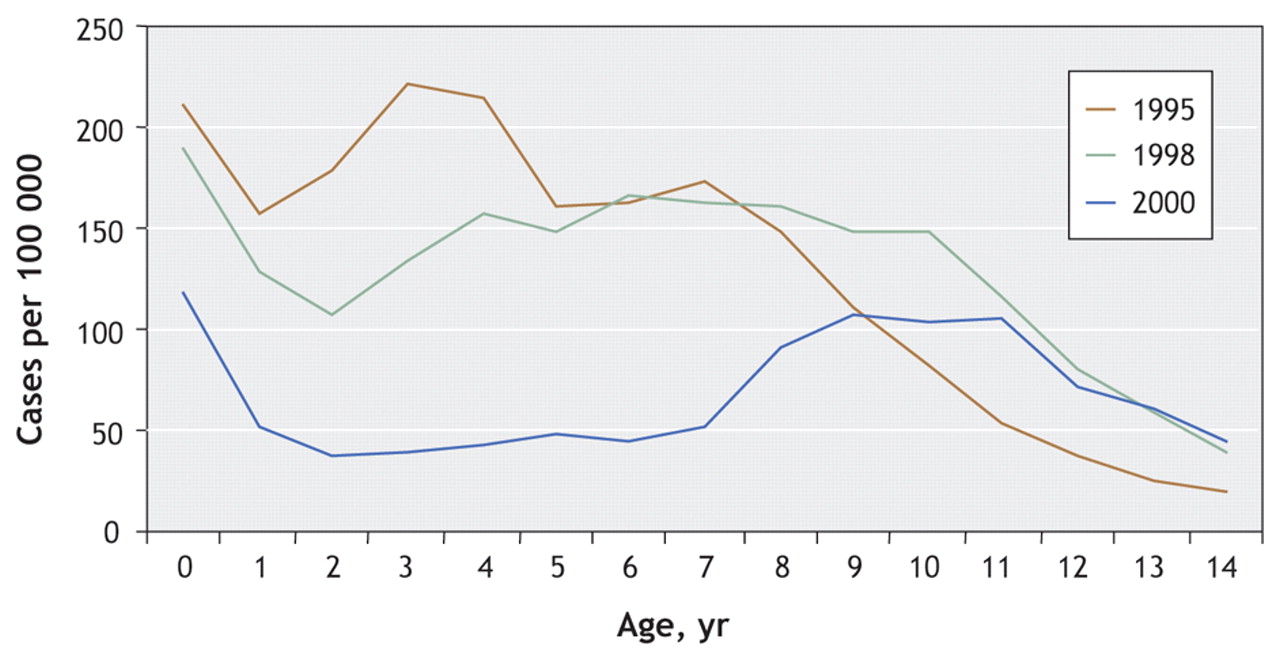
Fig. 3: Pertussis incidence by age among children in 4 provinces in 1995, 1998 and 2000. During the 1990s, excluding infants, the highest incidence was observed among children born between the late 1980s to early 1990s: in 1995, the highest incidence was observed among children 3 years of age, in 1998 among those 6 years of age and in 2000 among those 9 years of age.
Currently, Canadian children receive a combination vaccine of diphtheria and tetanus toxoids, acellular pertussis, inactivated poliomyelitis and Hemophilus influenzae type b (DTaP–IPV–Hib) at 2, 4, 6 and 18 months and a booster dose of DTaP–IPV between 4 and 6 years. Because of the recent upsurge in pertussis rates among adolescents, a booster dose of diphtheria–tetanus–acellular pertussis vaccine (dTap) has been offered to all Canadian adolescents since 2004.
Between 1989 and 2000, an average of 1113 (3.8 per 100 000) pertussis cases were admitted to hospital each year. The admission rate remained stable until 1995, when it began decreasing, reaching a low of 1.5 per 100 000 in 2000. Of cases admitted to hospital, 62% were under one year of age, for an average admission rate of 182.7 per 100 000 in this age group. Between 1991 and 2001, 89% of infants admitted to IMPACT hospitals (12 tertiary care pediatric hospitals across Canada) with pertussis were younger than 6 months of age. The ratio of reported cases to hospital separations increased from 1.1:1 in 1988 to 11.2:1 in 2000. The increase in this ratio is due in part to a shift in cases to older age groups and to the improved diagnosis and reporting of pertussis cases. The decrease in hospital admission rates in the last few years may be due in part to the greater efficacy of the acellular vaccine. However, infants who are not yet fully vaccinated remain at high risk of severe disease requiring hospital admission. Between 1989 and 2000, 19 pertussis-related deaths were reported. Of these, 16 (84.2%) were among infants, of whom all but one were younger than 3 months and of whom only one had been vaccinated.
The changing epidemiology of pertussis in Canada in the 1990s has led to the emergence of groups at higher risk of the disease: young infants, adolescents and adults. Cases admitted to hospital have shifted to infants younger than 6 months, and deaths are particularly high among infants younger than 3 months, who have few options for protection. Every effort should be made to vaccinate infants at the recommended age and to diagnose and treat pertussis in children and adults in contact with infants.
The recently implemented dTap immunization program for adolescents is expected to curb the increasing incidence in this age group. However, decreased circulation of Bordetella pertussis and waning immunity may lead to a continued increase in rates of pertussis among adults. To decrease the risk among adults and their contacts, the National Advisory Committee on Immunization recommends that all Canadian adults receive a single dose of dTap vaccine instead of a tetanus–diphtheria booster.
Footnotes
Competing interests: None declared.
In this issue
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

