


Cervical infection with high-risk (oncogenic) genotypes of human papillomavirus (HPV) is a necessary early event in cervical carcinogenesis; however, cervical cancer will not inevitably develop in women with such an infection. Therefore, high-risk HPV infection alone is not considered a sufficient cause of cervical cancer. Now that HPV testing is widely available, it is important for clinicians to understand the natural history of cervical intraepithelial neoplasia (CIN) and use this information to guide their recommendations to women regarding cervical cancer screening.

Fig. 1: Full spectrum of cervical carcinogenesis, showing the pre-invasive lesions that lie along the pathway from human papillomaviros (HPV) infection to cervical cancer. LSIL = low-grade squamous intraepithelial lesion, CIN 1 = grade 1 cervical intraepithelial neoplasia, HSIL = high-grade SIL, CIN 2–3 = grade 2 or 3 CIN.
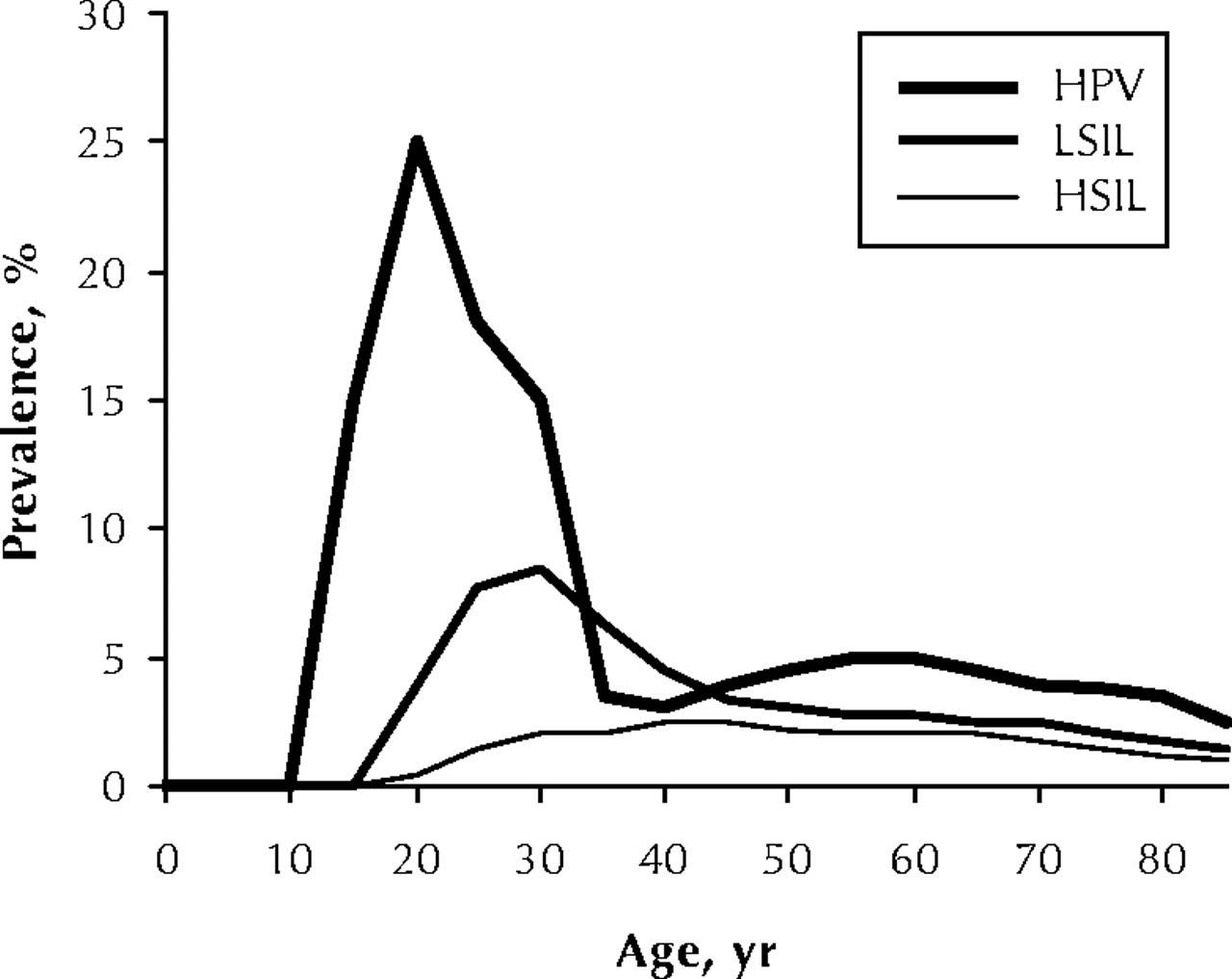
CIN represents the spectrum of pre-invasive lesions that lie along the pathway from HPV infection to cervical cancer (Fig. 1).1 The natural history of its cytologic counterpart, the squamous intraepithelial lesion (SIL), and of HPV infection has been shown to vary with the age of the affected woman (Fig. 2).2,3,4,5,6,7 In particular, the development, persistence, regression and progression of low-grade SIL (LSIL) seem to demonstrate the greatest variability as a function of age.8,9,10,11

Fig. 2: Prevalence of HPV infection, LSIL and HSIL by age.
Some investigators have stressed that adolescent females may be at increased risk of SIL because of differences in the biologic maturity of the immune system and cervix. In addition, the cervical ectopy and metaplastic changes in the transformation zone from puberty onward may increase the susceptibility of the cervix to HPV infection in the adolescent.12 These biologic changes in the cervix continue throughout a woman's lifetime, and thus it is difficult to speculate at what age these changes will alter the course of HPV infection or the behaviour of SIL. Most of the studies mentioned earlier have shown differences between “younger” and “older” women,2,3,4,5,6,7,8,9,10,11 but the the marked heterogeneity across investigations does not permit a simple interpretation of a process that is more likely to be gradual rather than a blunt change in risk patterns.
In the context of this commentary and our recommendations for HPV screening, we have defined “young” women as those aged 24 years or less. We chose this cut-off because the incidence of invasive cervical cancer is negligible among females 15–19 years old and very low (1.7 per 100 000 annually) among those 20–24 years old.13 In addition, studies involving females aged 13–22 years and those involving university students, described below, have shown relatively similar results in terms of the natural history of HPV cervical infection, LSIL behaviour and patterns of sexual activity.
In developing guidelines for screening women aged 24 years or less and for following those with abnormal test results, we had to examine the natural history of HPV infection. The prevalence of cervicovaginal high-risk HPV infection is high (up to 49%) among adolescent women.6 The overall median duration of high-risk HPV infection is about 13 months, with certain types persisting even longer.4 Women with persistent infection are more likely to acquire incident LSIL and persistent LSIL.11 The prevalence of LSIL among young women has also been shown to fluctuate between 2.5% and 7.7%.8,10,14 In addition, in women with high-risk HPV infection, LSIL regresses more slowly (mean 13.8 months) and progresses more quickly (mean time to HSIL or worse 73.3 months) than in women with other HPV genotypes.11 Despite these figures, it is generally accepted that both high-risk HPV infection and LSIL tend to be transient phenomena among young women. Moscicki and colleagues,9 in a longitudinal study involving adolescent women, showed that 91% of cases of LSIL had regressed at 36 months' follow-up.9 Even among women with high-risk HPV infection, 81% of the cases of LSIL had regressed and only 6% had progressed. For these reasons, conservative management of young women with LSIL should be encouraged.
The algorithm we have developed (Fig. 3) assumes that, despite the current recommendations for delaying cervical cytology screening until women have been sexually active for 3 years, some clinicians still perform the test much sooner for a variety of reasons that may be specific to the provider's perception of individual risk or may be contextual (e.g., opportunistic screening in the context of other health care interventions). The suggested algorithm incorporates the most recent recommendations of the American Society of Colposcopy and Cervical Pathology15 and the current evidence-based information pertaining to HPV infection and LSIL in young women.16 HPV testing refers exclusively to the existing commercial assay for DNA of high-risk genotypes of HPV.

Fig. 3: Algorithm for the management of immunocompetent women aged 24 years or less with cytologic evidence of LSIL. Pap = Papanicolaou smear, ASCUS = atypical squamous cells of undetermined significance, HR-HPV = high-risk HPV genotype.
Immunocompetent women aged 24 or less with LSIL whose first vaginal intercourse was within 3 years before screening can be managed with repeat cytology or HPV DNA testing in 12 months after the index abnormal cytologic result. The patient should be referred for colposcopy if the repeat cytology smear reveals atypical squamous cells of undetermined significance (ASCUS) or an abnormality of worse severity. If HPV DNA testing yields positive results, the patient should be referred for colposcopy, otherwise she should be asked to return for routine annual screening. The rationale for this arm of the algorithm is that the risk of progression to a high-grade precancerous lesion or cancer is exceptionally low among women who have been exposed to HPV for less than 3 years.16
Immunocompetent women aged 24 or less with LSIL whose first vaginal intercourse was 3 or more years before screening can be managed on the basis of whether they had any abnormal cytology smears previously. If they had no previous smears or had abnormal smears showing ASCUS or worse, they should be referred for colposcopy. The latter group may represent those with persistent cytologic abnormalities and HPV infection, which places them at increased risk of progression to high-grade lesions. For women with LSIL whose previous cytology smears were normal, there are again 2 options. One is to repeat the cytology test in 6 and 12 months and refer the patient for colposcopy if either of the 2 smears reveals ASCUS or worse; if the results of both repeat smears are normal, the patient should be asked to return for routine annual screening. The other option is to perform HPV DNA testing at 12 months after the index LSIL; if the results are positive, the patient should be referred for colposcopy.
After colposcopy, management should continue on the more conservative path, because the majority of biopsy-proven grade 1 CIN lesions in young women will resolve spontaneously within 2–3 years. In our algorithm, we do not encourage the use of HPV DNA testing in young women with LSIL whose subsequent cytology smear shows ASCUS; this recommendation is supported by findings in a review by Kahn and Hillard.17 Results of the well-known ASCUS/LSIL Triage Study (ALTS) showed that HPV DNA was detected in 83% of the women with LSIL.18 Given that the median duration of high-risk HPV infection is greater than 13 months, repeating DNA testing in women whose smears show ASCUS will unlikely lower the overall referrals to colposcopy significantly.11 Also, very few institutions offer HPV DNA testing free of charge to the patient; adolescent and young women are less likely to be able to afford the cost of this test.
In following our algorithm, clinicians have a good opportunity for education and promotion of preventive health care. These benefits are more difficult to measure on a financial level. Although the evidence is weak, women with LSIL should be advised to stop smoking because of the possible role it plays in the persistence and progression of cervical lesions.19 Likewise, condom use should be advised, because it promotes regression of CIN lesions and clearance of HPV infection.20,21
Research into cervical cancer prevention has progressed faster than that into most other oncological fronts. Readers are no doubt aware of the recent, promising results of prophylactic HPV vaccines.22 Licensed HPV vaccines may be a reality within 2–5 years, and their public health benefit will probably influence future revisions of the above recommendations.
Knowledge of the cancer-causing potential of HPV genotypes is also constantly increasing. The International Agency for Research on Cancer was responsible for a large epidemiologic investigation that provided strong evidence for the association of up to 18 high-risk HPV genotypes with cervical cancer.23 The same agency recently listed 13 HPV genotypes as group 1 carcinogens in its monograph series24 but emphasized the substantial diversity among them with respect to cervical cancer risk. In particular, HPV 16 seems to merit individual consideration because of its stronger propensity to persist and to lead to neoplastic changes than other high-risk HPV genotypes.25 There is currently no clinical indication for HPV typing. However, given current research trends, one should not be surprised if more complex screening and management algorithms based on HPV testing and typing find their way into clinical practice in the future.
Footnotes
-
Contributors: Both authors contributed to the concept and writing of the manuscript and approved the final version to be published.
Competing interests: None declared.
References
In this issue
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

