


- © 2004 Canadian Medical Association or its licensors
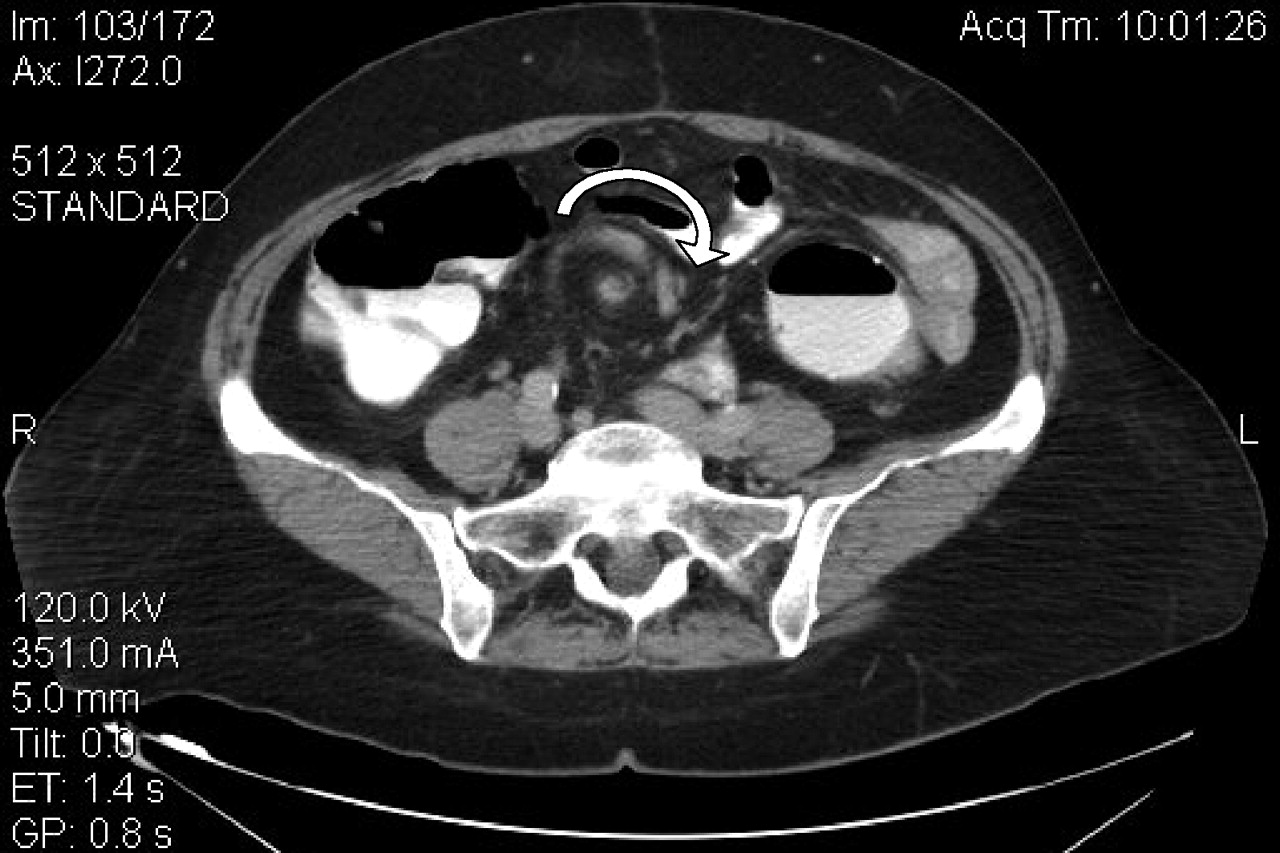
A 61-year-old woman presented to the emergency department with acute abdominal pain of several hours' duration accompanied by nausea but no vomiting. Her past medical history was significant for adenocarcinoma of the sigmoid colon treated with surgical resection 4 years before, after which she presented on multiple occasions to her surgeon with abdominal pain. Upper and lower gastrointestinal endoscopies had failed to identify a cause for her symptoms. At current presentation she was in obvious pain. Her heart rate was 105 beats/min, blood pressure 170/90 mm Hg, and she was afebrile. Bowel sounds were present on abdominal examination, as was tenderness in the periumbilical region, but there was no guarding or rebound tenderness. The remainder of her examination was unremarkable. Results of blood work and urinalysis were normal, as were abdominal radiographs. She received treatment for pain overnight, but her symptoms persisted. A triple contrast-enhanced abdominal CT scan revealed a 540° twist of the small-bowel mesentery, which is shown by the clockwise whirl-like pattern around the axis of the superior mesenteric artery in Fig. 1. Our patient immediately underwent a laparotomy with lysis of adhesions caused by her previous hemicolectomy and detorsion of the affected bowel loop. The bowel appeared mildly ischemic but viable. Her recovery was uneventful, with full resolution of abdominal pain.
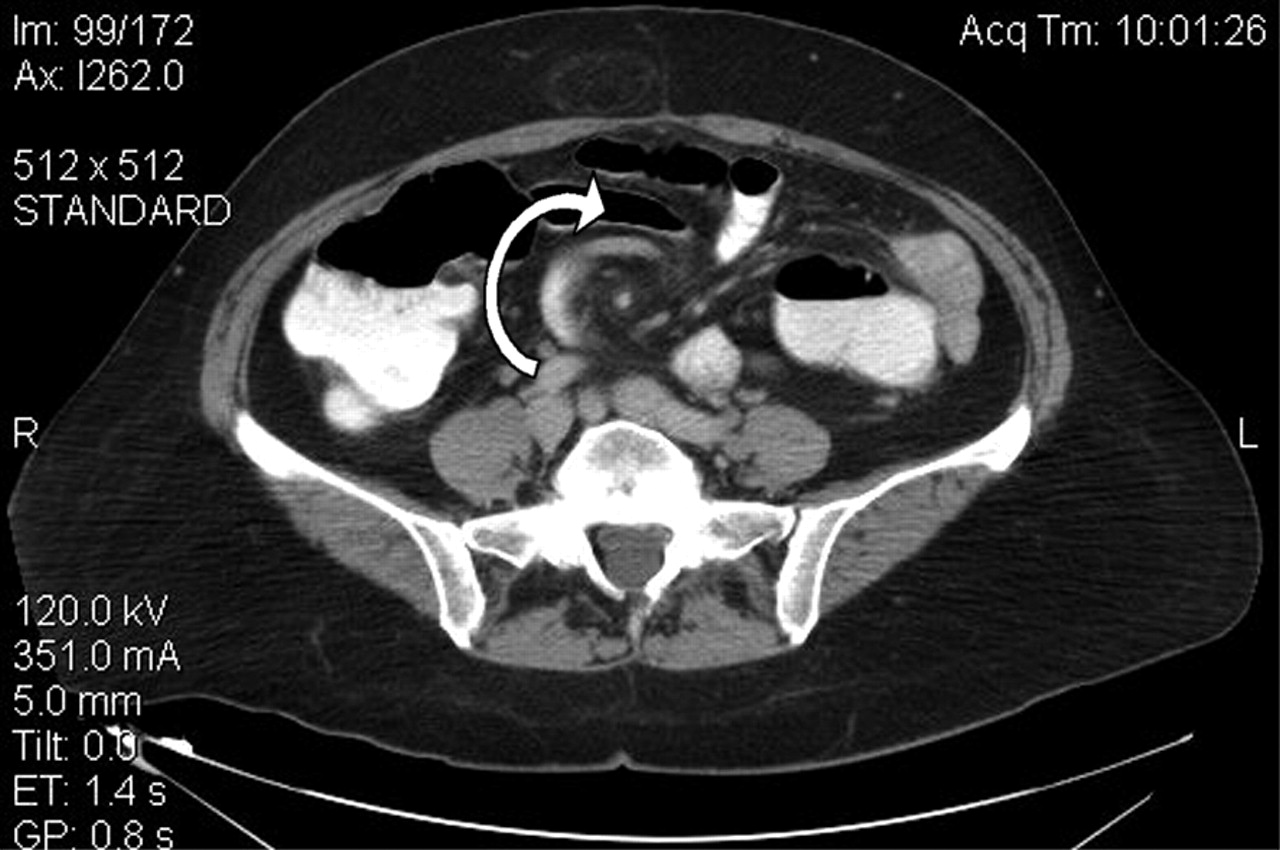

Figure 1. Continued.

Figure 1. Continued.
Small-bowel volvulus (SBV) refers to the abnormal twisting of a loop of small bowel around the axis of its own mesentery, which produces a mechanical bowel obstruction.1 SBV may also result in torsion and occlusion of the mesenteric vasculature, which can lead to bowel ischemia and ultimately necrosis.2 Mortality for SBV has been estimated to be 9%–35%, but this increases to 20%–100% with bowel necrosis.3,4 In North America and western Europe, the annual incidence is 1.7–5.7 cases per 100 000, but rates of 24–60 per 100 000 have been observed in Africa, Asia, the Middle East and India;3,4 the higher rates are thought to be related to dietary practices (e.g., the ingestion of large volumes of fibre-rich food after periods of prolonged fasting).5 Primary SBV occurs primarily in children with normal gastrointestinal anatomy from the high-incidence regions listed above, and secondary SBV is caused by anatomical anomalies (e.g., midgut malrotation) or acquired lesions (e.g., postsurgical adhesions).3,4
Diagnosis may be difficult since the symptoms of abdominal pain, nausea and vomiting are nonspecific.4 The most important clue is a recent history of intermittent, recurring abdominal pain that is usually periumbilical or epigastric and which may occur after ingestion of a meal.1,2 The severity of pain is directly related to the duration of vascular compromise but unrelated to the degree of intestinal obstruction.4 Peritoneal irritation, although a marker for urgent laparotomy, is also nonspecific and is estimated to be present in only a quarter of patients with SBV.4 Laboratory tests are equally nonspecific, and elevations of leukocyte counts and transaminase, amylase and lactate levels may occur inconsistently. Plain radiographs may be normal or suggest bowel obstruction, but it is difficult to differentiate between SBV and other causes of obstruction that may resolve with conservative management. Thus, the imaging modality of choice is CT scanning.2,3 Surgery is the mainstay of treatment, and it is required urgently in cases of suspected impending bowel necrosis.3
Peter G. Katis Assistant Medical Director Emergency Medicine University Health Network Lecturer Department of Family and Community Medicine University of Toronto Solange M. Dias Family Medicine University of Toronto Toronto, Ont.
In this issue
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

