


A 54-year-old woman was referred to the endocrinology service for evaluation of thyromegaly detected incidentally on physical examination. She was asymptomatic at the time, but 48 months earlier she had been found to have estrogen/progesterone receptor-negative infiltrating ductal breast carcinoma and had known bone metastasis. On examination, her thyroid was diffusely enlarged to about 3 times normal size and was firm and nontender with no distinct nodules. The remainder of her examination was unremarkable. Her thyroid stimulating hormone (TSH) level was normal (2.5 mIU/L); free thyroxine was not measured, and antithyroid peroxidase and antithyroglobulin antibody levels were not elevated. Ultrasonography of the neck showed both thyroid lobes enlarged, with isoechoic nodules (3.6 х 2.2 х 2.0 cm) in each lobe and lymphadenopathy in inferior jugular chains bilaterally. Fine-needle aspiration of one of the nodules and a lymph node revealed malignant cells in an inflammatory background consistent with metastatic carcinoma (Fig. 1A). The cells had similar features to cells from a previous fine-needle aspiration of breast carcinoma performed when cancer was first diagnosed (Fig. 1B).

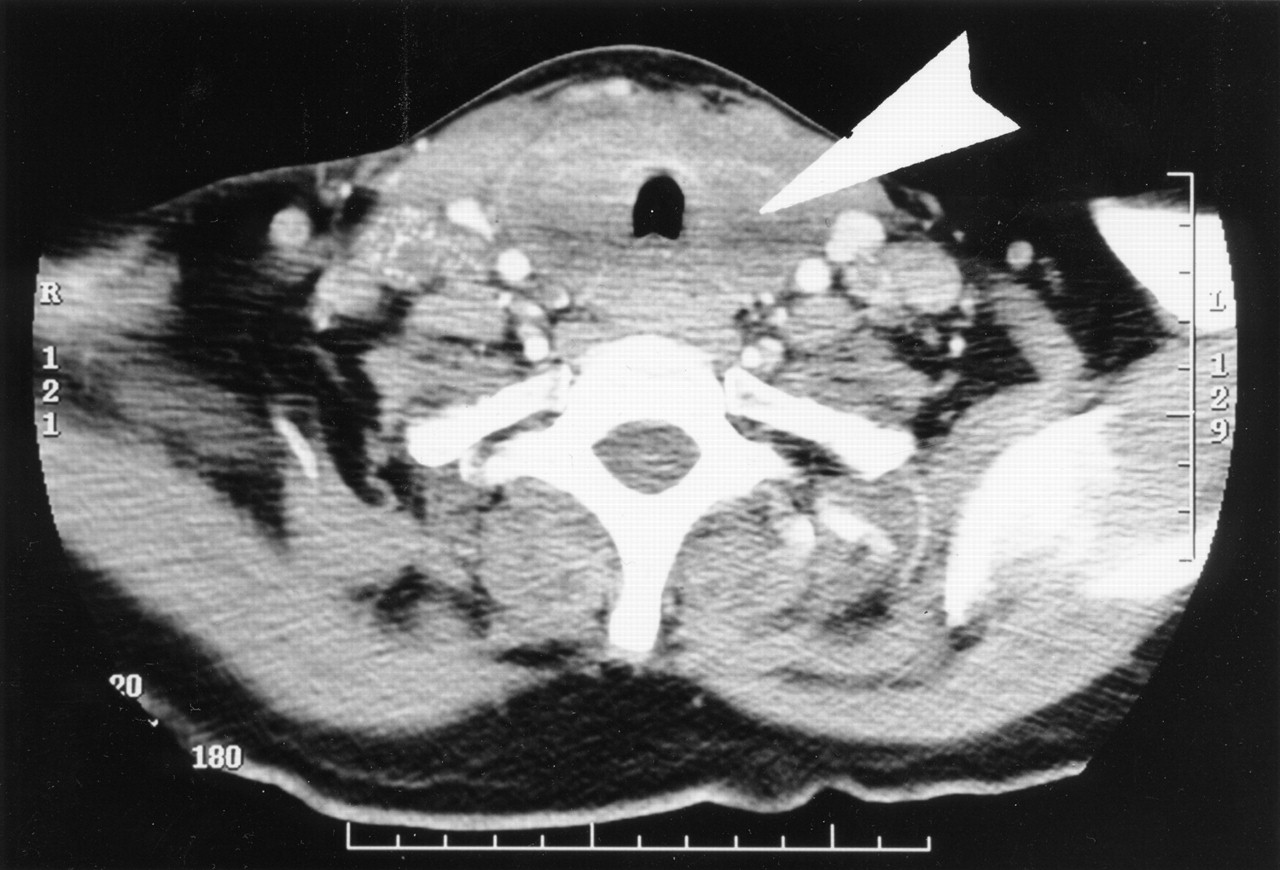
The patient experienced progressive dysphagia, hoarseness of voice and weight loss over the next few months, and a CT scan taken 4 months after the initial assessment showed significant thyromegaly with encasement of the trachea (Fig. 2). The TSH level was elevated (56 mIU/L) and the free thyroxine level was 6.6 (normally 9.0–19.0) pmol/L. These findings were consistent with hypothyroidism, and the patient was given levothyroxine. Her TSH level 4 weeks later was 2.4 mIU/L. She was not considered a surgical candidate and received palliative radiotherapy to the neck. She noticed a transient improvement in her symptoms but succumbed 2 months later to her progressive metastatic disease.
Metastases to the thyroid gland are uncommon, with a reported prevalence of 0.5%–2% in all cancers.1 The most common malignant diseases to metastasize to the thyroid include breast, lung and renal cell carcinoma. Such metastases generally occur in the setting of widespread known metastatic disease, but involvement of the thyroid may be the initial manifestation of an underlying malignant disease.2 Thyroid metastases may either be asymptomatic or present with diffuse or nodular goitre, pain or symptoms such as dysphagia, stridor and hoarseness of voice arising from compression of the esophagus, trachea and recurrent laryngeal nerves respectively. Mean survival after detection of metastases to the thyroid has been reported to be 5 months. Differentiation between benign thyroid disease, primary thyroid cancer and metastases can be challenging, and either fine-needle aspiration or thyroidectomy is required for definitive diagnosis.3
Although destructive thyroiditis leading to transient hyperthyroidism in patients with thyroid metastases has been described,4 hypothyroidism due to thyroid metastases is extremely rare. In addition to causing the thyroid enlargement and nodule formation, we believe that the thyroid metastases were responsible for our patient's hypothyroidism, because she became significantly hypothyroid in a short period and had negative antithyroid antibody levels.
Physicians should consider the possibility of metastatic disease to the thyroid when evaluating patients with evidence of thyroid dysfunction, particularly if they have a history of malignant disease.
Hasnain M. Khandwala Division of Endocrinology Department of Medicine Rajni Chibbar Department of Pathology University of Saskatchewan Saskatoon, Sask.
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

