


A CMAJ editorial1 published in May 2003 cites the case-fatality rate for severe acute respiratory syndrome (SARS) in Canada as 12.4%. We have been examining death rates in Taiwan, Canada and Hong Kong2,3,4,5,6 and have found significant variation over time (Fig. 1, next page).
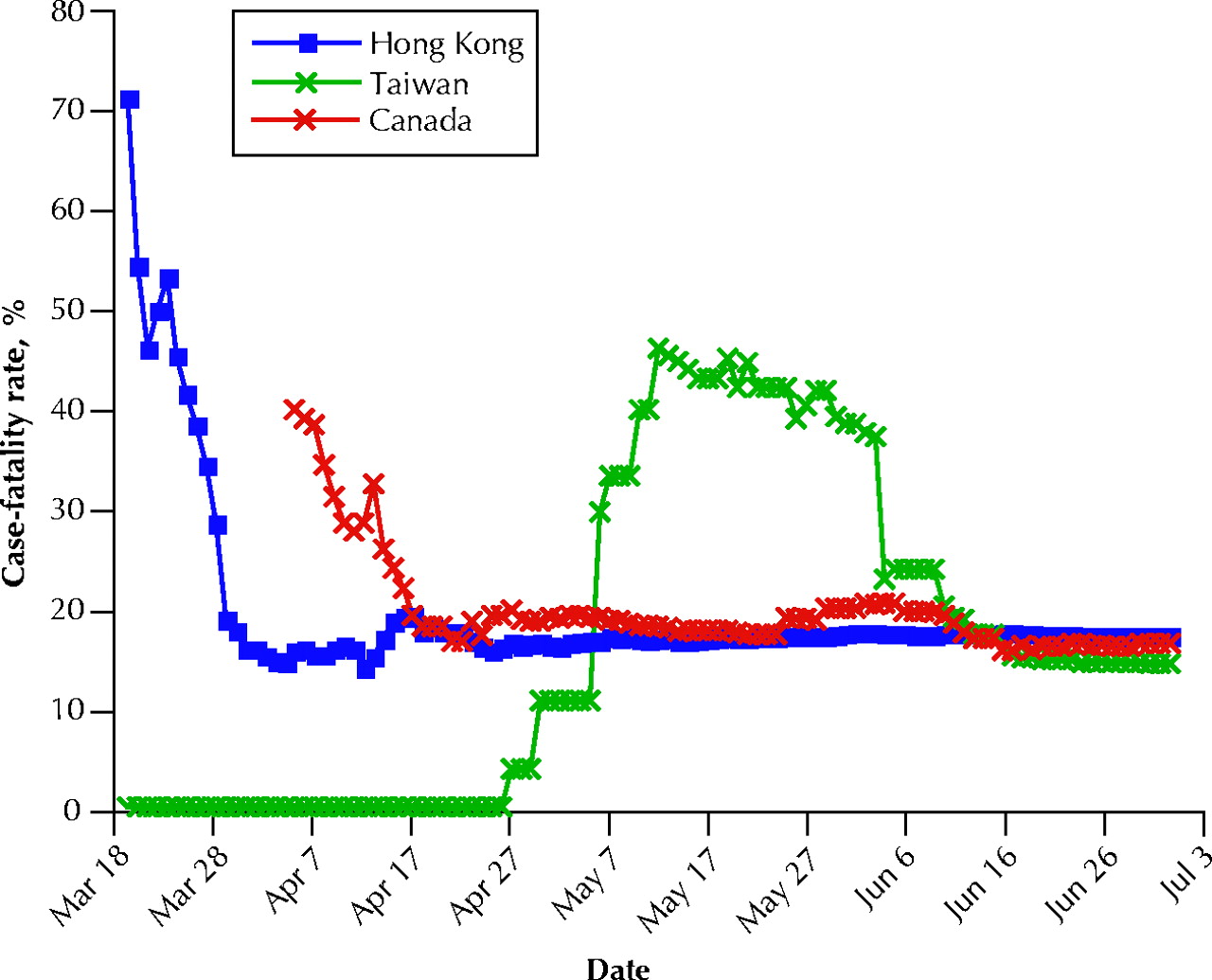
In Taiwan the first case of SARS was reported on Mar. 14, 2003;7 there were 78 cases by the end of April and 676 cases by the end of May.6 The first death was reported on Apr. 27, at which time the case-fatality rate (the number of deaths divided by the sum of deaths and recoveries) was only 3.8%. However, in mid-May the case-fatality rate rose markedly to a peak of about 45% and then stabilized at about 15% in June.
In Canada the first case of SARS was reported on Feb. 23 and the first 10 deaths were reported on Apr. 7. The case-fatality rate on that date was 38.5%; it fell to about 20% by the end of April and stabilized at about 17% in late June.
Finally, in Hong Kong case-fatality rates were very high (about 71%) early in the outbreak but later fell to about 17%.
According to recent data from Hong Kong,8 hospital death rates among patients at least 60 years of age peaked sharply at about 12 days after admission, whereas younger patients showed maximal (and lower) peak death rates at about 18 days. Thus, to understand the differences in case-fatality rates over time and between countries it is important to take age into account. Another factor that might explain initially high rates is physicians' lack of clinical experience with the disease early in the outbreak. Published reports9,10 suggest wide variation in therapy, which might also affect outcome. In addition, there has been considerable speculation that there may be different genetic forms of the virus (i.e., different degrees of virulence for the same virus) or that the virus has become less virulent over time.
Wing K. Fung Philip L.H. Yu Department of Statistics and Actuarial Science The University of Hong Kong Hong Kong, China
In this issue
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

