


Technology: Nasal continuous positive airway pressure (CPAP) for chronic congestive heart failure
Use: Nasal CPAP uses a blower pump to generate continuous positive air pressure and a nasal mask to apply it to the airways (Fig. 1). For patients with congestive heart failure, the positive pressure inflates the pharynx and lungs and applies external pressure to the heart.

Fig. 1: Patient using a nasal continuous positive airway pressure (CPAP) apparatus for sleep apnea.
History: CPAP has been in use for over 50 years, mainly for weaning patients from mechanical ventilation. For this purpose it was applied by way of an endotracheal tube or full face mask. In 1981, Sullivan and associates1 described the use of a nasal mask so that CPAP could be applied more conveniently and comfortably. They first used nasal CPAP to treat obstructive sleep apnea, whereby the air pressure acts as a pneumatic splint to prevent pharyngeal collapse during sleep. Nasal CPAP is now widely used at home for this indication.
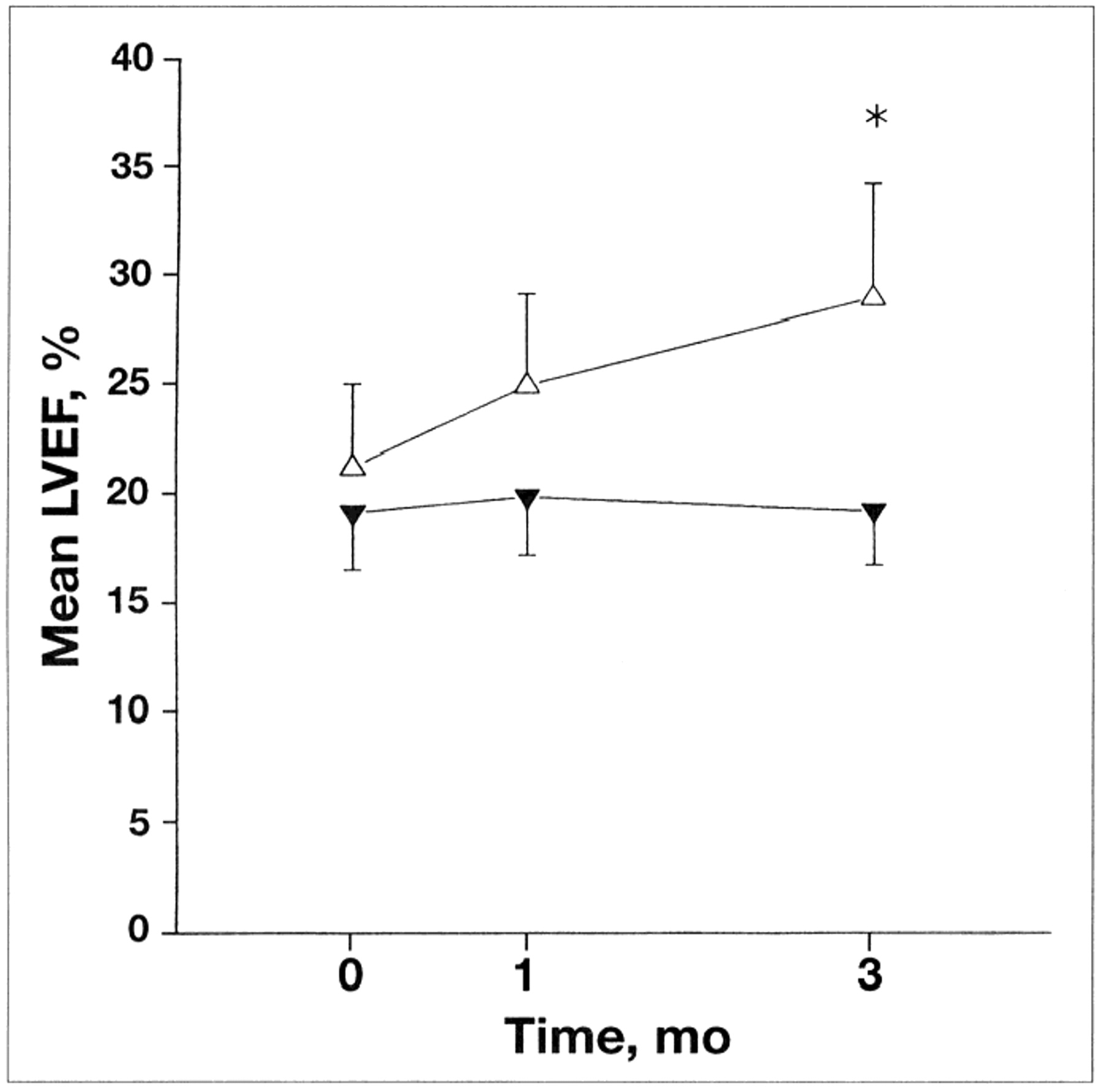
More recently, my colleagues and I realized that nasal CPAP might be useful in patients with chronic congestive heart failure. Our rationale was that CPAP would increase intrathoracic pressure and thereby reduce the left ventricular preload and afterload. In patients with congestive heart failure and central or obstructive sleep apnea, CPAP would have the added benefit of treating the apnea and apnea-related hypoxia, and of improving sleep quality. We first described its use for sleep apnea and congestive heart failure in 1989.2 In this and subsequent randomized trials, we found that it alleviated the apnea and increased the left ventricular ejection fraction (Fig. 2), that it reduced functional mitral regurgitation, and atrial natriuretic peptide and norepinephrine levels,[2–4] and that it decreased the hospital admission rate.2 In 1991 we described a relation between idiopathic dilated cardiomyopathy and obstructive sleep apnea. The abolition of obstructive sleep apnea by nasal CPAP led to significant improvement in the left ventricular ejection fraction.5 In all of these studies the patients tolerated CPAP well and did not report serious side effects.

{kind=link}
{kind=link}
Fig. 2: Effect of CPAP on left ventricular ejection fraction (LVEF) in patients with congestive heart failure and central sleep apnea. Values shown are means and standard errors of the mean. After 3 months, LVEF was significantly greater in treatment group (▵) than in control group (▾) (*p = 0.019). Reproduced from Naughton et al,3 with permission. © American Lung Association
The beneficial effects of nasal CPAP in congestive heart failure are probably due to 3 mechanisms. First, CPAP increases intrathoracic pressure and lowers left ventricular transmural pressure (afterload). It thereby acts as a cardiac assist device to augment cardiac output in patients with elevated left ventricular filling pressure.4 Second, in patients with congestive heart failure who have central or obstructive sleep apnea, CPAP abolishes nocturnal blood pressure surges by eliminating the apnea. Third, CPAP reduces activity of the sympathetic nervous system by alleviating apnea-related hypoxia and preventing arousals from sleep. Because these mechanisms of action depend on the generation of positive intrathoracic pressure, they differ fundamentally from, and are additive to, the effects of optimal drug therapy for congestive heart failure.[3–6]
Promise: Cheyne-Stokes respiration with central or obstructive sleep apnea has been found to occur in about 50% of patients with chronic congestive heart failure whose left ventricular ejection fraction is less than 45%.[7, 8] Therefore, many such patients should benefit from CPAP. In addition to CPAP being safe and well tolerated, it shows promise of improving cardiovascular function and possibly improving survival in a substantial proportion of patients with congestive heart failure.
Problems: Sleep apnea is common in patients with congestive heart failure,[7, 8] is associated with increases in afterload, sympathetic nervous system activity and mortality,[4–6, 9] and is amenable to therapy with CPAP.[2–5, 7] Despite the rapidly growing body of evidence on which these statements are based, there are few reports on the use of CPAP and other forms of positive airway pressure to treat sleep apnea in patients with congestive heart failure. This suggests that the adverse effects of sleep apnea in such patients, and of the potential benefits of CPAP in their management, are not widely recognized.
Prospects: In an effort to find more compelling evidence of CPAP's benefits in patients with congestive heart failure, the Canadian Positive Airway Pressure Trial is currently under way in 8 centres across Canada. [The list of trial investigators and information about the eligibility criteria and study protocol appear in the online edition (www.cma.ca/cmaj/vol-162/issue-4/0535app1.htm]. If this trial or others similar to it demonstrate that CPAP reduces mortality and cardiac transplantation rates, then its efficacy for the treatment of congestive heart failure will have been established.
Competing interests: None declared.
The work was funded by operating grants MT 11607, MA 12422 and UI 14909 from the Medical Research Council of Canada.
Acknowledgments
Conference themes include:
• Pathways
• Evaluation of interventions
• Methodology
• Policy and collaborative efforts
• Populations at risk (children and adolescents, women including pregnant women, minorities)
• Forum (constructive criticism of recently published research)
The official languages of the conference will be English and Spanish.
For more information, please contact
Dr. Barbara Starfield; School of Public Health; Johns Hopkins University; Room 452; 624 N Broadway; Baltimore, MD 21205; bstarfie{at}jhsph.edu
Dr. Jose Maria Paganini; Facultad de Ciencias Medicas; UNLP; 1er Piso Edificio de la Biblioteca; Calle 60 y120; 1900 La Plata, Argentina; isequity{at}netverk.com.ar
In this issue
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
Similar Articles
Collections

