


Abstract
Background: Although much has been written about hormone replacement therapy (HRT), there are few clearcut recommendations on its use. The purpose of this study was to determine Ontario physicians' patterns of and reasons for prescribing HRT, their use of pretreatment investigations and their surveillance of HRT users, and to determine whether physicians' reported practice is consistent with existing recommendations.
Methods: A self-administered questionnaire was mailed to a nonproportional stratified sample of 327 Ontario physicians (23.9% gynecologists, 76.1% general practitioners/family physicians [GP/FPs]). Outcome measures were ranking of reasons for prescribing HRT, nature of preliminary testing, regimens prescribed, duration of HRT and frequency of follow-up.
Results: The response rate was 60.9% overall (70.9% of the gynecologists, 58.3% of the GP/FPs). Prevention of osteoporosis was reported by 97.4% as an important or very important reason for prescribing HRT; prevention of coronory artery disease was important or very important for 89.3%. When considering whether or not to prescribe HRT, 97.3% stated that breast cancer was an important or very important factor. When presented with hypothetical cases, 97.0% stated that they would prescribe combined estrogen-progestin for a symptomatic woman with an intact uterus; 13.6% stated that they would do so for a woman with no uterus. Most reported that they would prescribe HRT for 12 or more years (73.3%) and would follow up patients every 1 to 2 years (70.6%).
Interpretation: Despite controversy about HRT in the published literature, the Ontario physicians surveyed reported similar reasons and patterns of prescribing, pretreatment investigations, and surveillance of postmenopausal women using HRT. These results suggest that Ontario physicians' knowledge about HRT is consistent with recommendations in the published literature.
Although 17 practice guidelines on hormone replacement therapy (HRT) have been developed[1–17] and several physician surveys[18–28] and review articles[29–30] have been published on the topic, there are few clearcut recommendations on when to prescribe HRT, which pretreatment investigations to conduct, which regimens to prescribe, how long HRT should be prescribed or what schedule of surveillance should be followed.
Most agreement in the literature appears to be about the benefits of estrogen in preventing osteoporosis and fractures.[14, 16, 17] There is some question about the benefits in preventing coronary artery disease (CAD). Observational studies suggested that the risk of CAD among estrogen users was about 30%-50% the risk among women not using estrogen.[29, 30] However, in a subsequent randomized controlled clinical trial involving women with CAD, the rate of CAD events was not reduced.31
The practice of physicians in this climate of uncertainty is unknown. We therefore surveyed a random sample of Ontario physicians to determine their patterns of and reasons for prescribing HRT, their use of pretreatment investigations and their surveillance of HRT use, and to determine whether these patterns are consistent with existing recommendations.
Methods
We obtained a list from the College of Physicians and Surgeons of Ontario of all physicians licensed with the college. Using a sample size calculation designed to provide 95% confidence intervals of 5%,32 we selected a nonproportional stratified sample of gynecologists and general practitioners/family physicians (GP/FPs) that allowed us to oversample gynecologists (25% gynecologists and 75% GP/FPs).
Physicians were considered ineligible if they had retired, were not currently seeing patients (e.g., were ill or on maternity leave), did not have their own practice (e.g., did locums only) or were not treating perimenopausal or postmenopausal women for gynecologic or primary care (e.g., practised only emergency medicine).
A mailed, self-administered questionnaire (available upon request from the authors) was developed to ascertain factors considered by respondents as important or very important for prescribing HRT and various aspects of their patterns of prescribing HRT (e.g., clinical workup, formulations prescribed and frequency of monitoring). Because a woman's menopausal status and the presence of risk factors may affect whether a physician considers prescribing HRT and the way it is prescribed,[19, 20, 22, 24, 26, 27] we included 3 hypothetical cases in the questionnaire: one in which a healthy 51-year-old woman with an intact uterus is experiencing severe menopausal symptoms, a second in which a healthy 54-year-old woman has no menopausal symptoms and a third in which a 40-year-old woman had undergone a hysterectomy and bilateral oophorectomy. The questionnaire provided a list of reasons for prescribing HRT, and physicians were asked to rate their importance using a 5-point Likert scale. Physicians were also asked to indicate pretreatment investigations they conduct or order when considering HRT, which hormonal regimens they would prescribe, the duration for which they would prescribe HRT and how often they would ask a woman to return for follow-up. Questions on physician and practice characteristics were also included.
The questionnaire and cover letter were pretested with 3 gynecologists, an internist and 9 GP/FPs. Revisions were made in accordance with their recommendations. We sent 2 mailings and a reminder postcard and telephoned nonrespondents using established survey techniques.33 Approximately 2 weeks after the initial mailing a reminder postcard was sent to all physicians. Follow-up packages were sent to nonrespondents 1 month after the initial mailing, and telephone calls were made approximately 1 month subsequent to the second mailing. Nonrespondents were contacted by telephone once.
Nonrespondents were compared with respondents by age, sex and years since graduation from medical school using a χ2 test of significance or a t-test for independent sample means. To describe the most important reasons for prescribing HRT, the "important" and "very important" categories were combined.
Because gynecologists were oversampled, the results were weighted when combining the 2 strata; this enabled each stratum to be represented in the same proportion as it is in the total population.34 When strata were analysed separately or when the characteristics of the sample were examined, weighting was not used.
Results
The number of usable questionnaires received was 327 (78 [23.9%] were gynecologists and 249 [76.1%] GP/FPs). Of the 125 gynecologists and 575 GP/FPs sent packages, 15 and 148 respectively were found to be ineligible or could not be contacted. Among the remainder, the response rate was 60.9% overall (70.9% for the gynecologists and 58.3% for the GP/FPs). The respondents and nonrespondents did not differ significantly by age, sex or years since graduation from medical school.
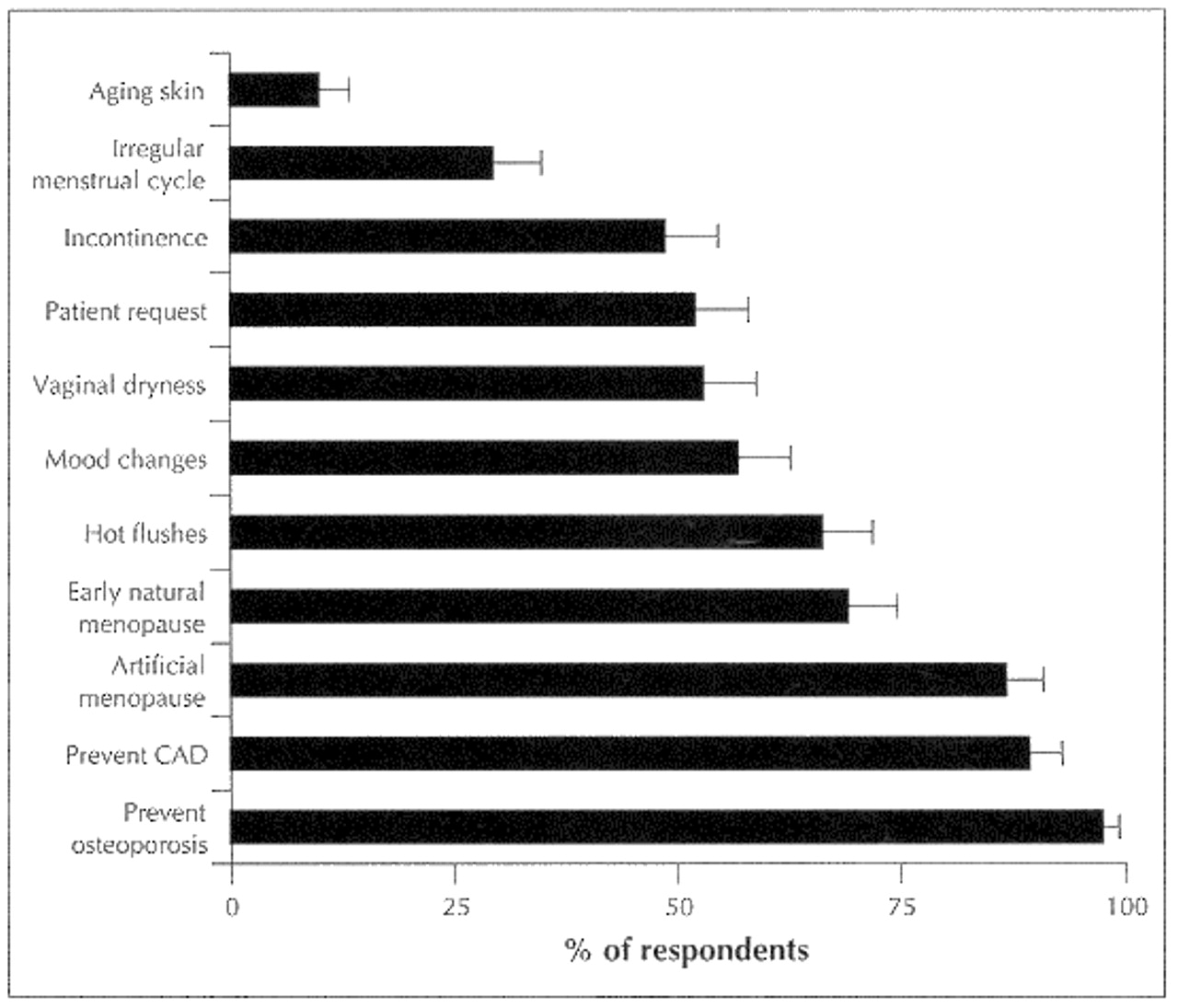
Nearly all (98.5%) of the respondents stated that they prescribe HRT. Prevention of osteoporosis was reported most often (by 97.4%) as an important or very important reason for prescribing HRT (Fig. 1). Other important factors were prevention of CAD (by 89.3%), and artificial and early menopause (by 86.8% and 69.1%, respectively).
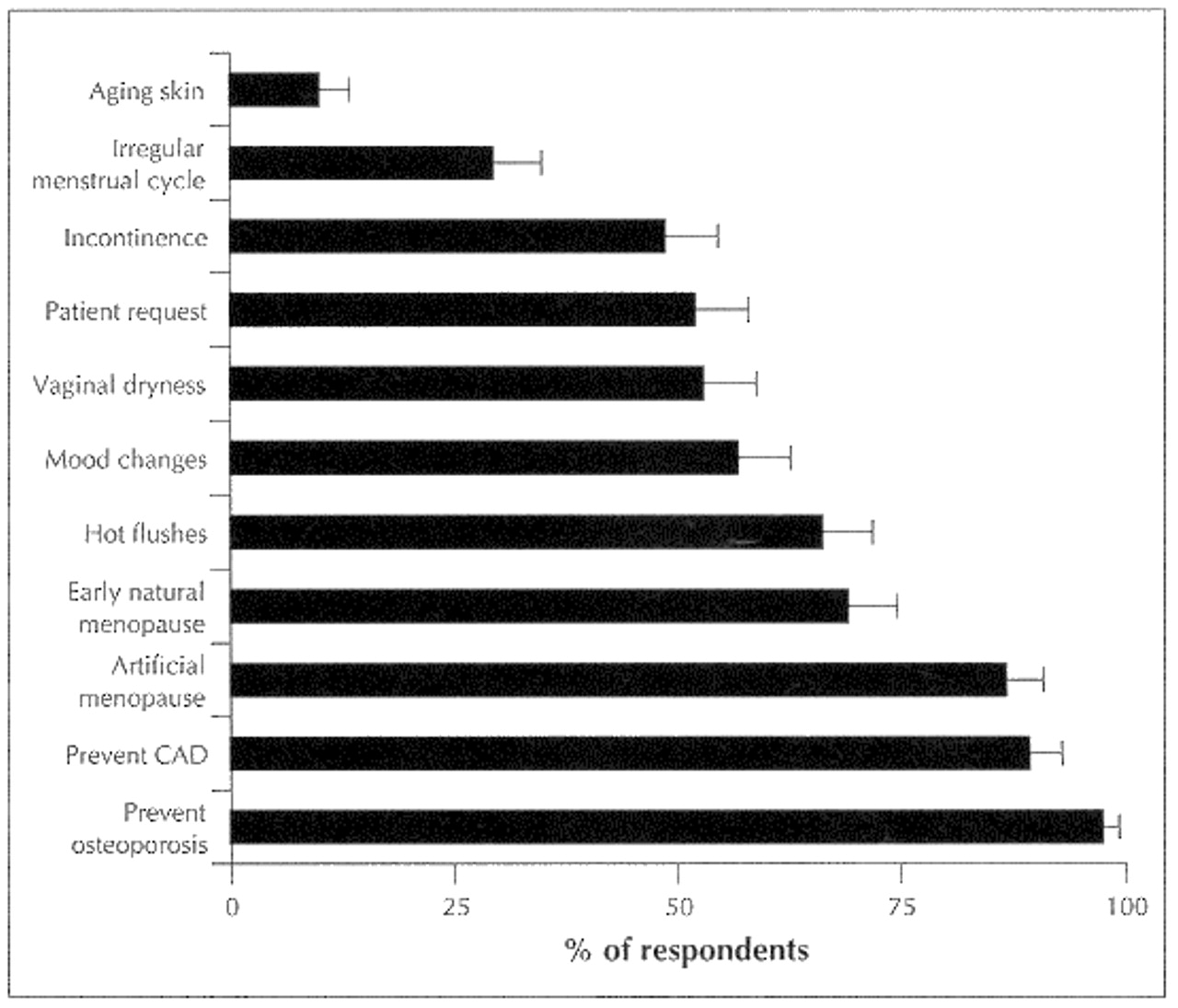
Fig. 1: Reasons for prescribing hormone replacement therapy presented to a sample of Ontario gynecologists and general practitioners/family physicians. Bars indicate proportion of respondents who rated each reason as important or very important; error bars indicate 95% confidence intervals (CIs). CAD = coronary artery disease.
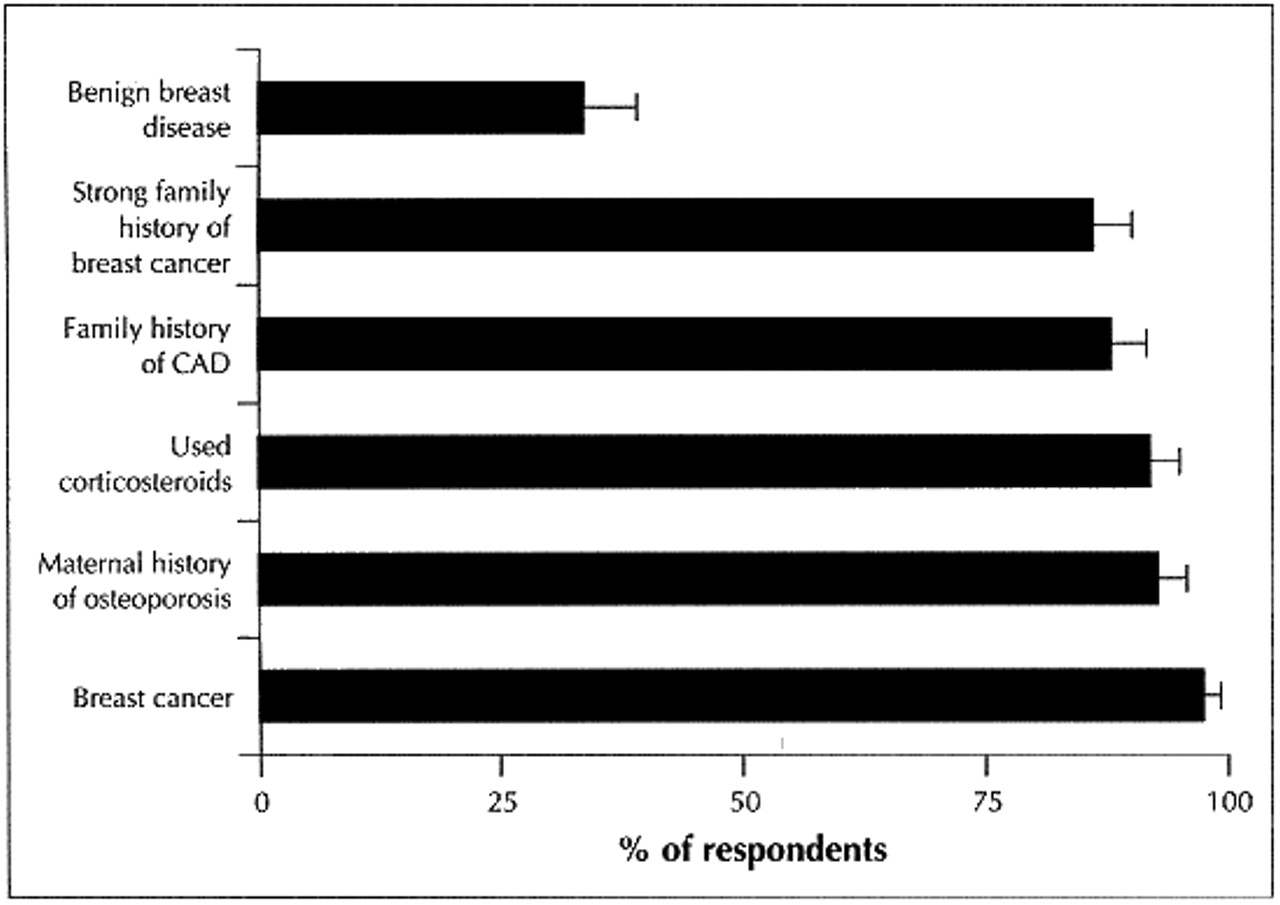
When considering whether to prescribe HRT in the case of the menopausal woman without symptoms, most physicians (97.3%) stated that breast cancer was an important or very important factor; other important factors included a maternal history of osteoporosis (92.6%) and a family history of CAD (87.8%) (Fig. 2).

{kind=link}
{kind=link}
Fig. 2: Factors considered important by respondents in the hypothetical case of a 54-year-old menopausal woman (no menstruation for 12 months) without menopausal symptoms. Bars indicate proportion of respondents who rated each factor as important or very important; error bars indicate 95% CIs.
The tests and procedures that respondents indicated they would perform are listed in Table 1. As for HRT regimens, most (97.0%) of the respondents reported that they would prescribe a combined estrogen-progestin formulation in the case of the woman with an intact uterus who was experiencing menopausal symptoms (Table 2). Only 1.3% stated that they would not prescribe progestin in this case. Although most of the respondents stated that they would prescribe estrogen alone in the case of the 40-year-old woman who had had a hysterectomy and oophorectomy, 13.6% reported that they would prescribe combined estrogen-progestin (Table 2). A large majority reported that they would prescribe HRT for 12 or more years (73.3%) and that they would follow patients up every 1 to 2 years (70.6%).
Table 1: Tests or procedures that respondents reported they would perform or order before prescribing hormone replacement therapy (HRT)
Table 2: HRT formulations considered by respondents in 2 hypothetical cases
Interpretation
Our survey findings indicate that the vast majority of Ontario physicians are familiar with the benefits of HRT described in the medical literature and practice guidelines (protection against osteoporosis, fractures and CAD) and risks from long-term use (endometrial and breast cancer). Nearly all of the respondents considered the prevention of osteoporosis and the presence of risk factors for osteoporosis (long-term use of corticosteroids and maternal history of osteoporosis) as important or very important reasons for prescribing HRT.
Almost 90% stated that they would prescribe HRT to prevent CAD and that a family history of CAD is an important factor. Although observational studies have consistently shown that estrogen protects against CAD,[29, 30] a recent randomized, blinded, placebo-controlled trial involving menopausal women with CAD found that a combined estrogen-progestin regimen did not reduce the overall rate of CAD events.31 Although that trial assessed HRT as secondary prevention, its findings will probably result in a re-evaluation of the role of estrogen in the prevention of heart disease.35 Our survey was conducted before publication of this clinical trial.
Breast cancer and a strong family history of breast cancer were considered contraindications for prescribing HRT by a large majority of the respondents. Although still controversial, studies suggest an increased risk of breast cancer among women receiving HRT.30
Few of the respondents chose a formulation other than combined estrogen-progestin in the case of the menopausal woman with an intact uterus. Thus, most of the physicians surveyed were consistent with the epidemiological literature30 and practice guidelines,[8, 16, 17] which recommend combined HRT for women who have an intact uterus and are at risk of endometrial cancer.
For cases in which a woman has had a hysterectomy, some practice guidelines indicate that it is unnecessary to prescribe combined HRT;[8, 16, 17] about 15% of the respondents do not appear to be following this recommendation. This is of concern because questions about the long-term effects of progestin and its role in CAD are unanswered. These respondents may have chosen the combined regimen because of a miscomprehension of the role of progestin in prevention, a possible misreading of the survey question, a lack of complete knowledge regarding the benefits and risks of HRT or some perceived benefit of progestin. Nevertheless, this practice was less frequent than that found in other studies. Ross and colleagues20 reported that 47% of physicians surveyed prescribed progestin to women without a uterus, and Brett and Madans36 reported that 20%-30% of women who had undergone a hysterectomy were prescribed combined estrogen-progestin therapy.
Our study had limitations. The overall response rate was about 61%. Although it might be argued that the respondents were not representative of the target population of Ontario gynecologists and GP/FPs, the respondents and nonrespondents were similar in age, sex and number of years in practice. Reliability and validity of the questionnaire were not tested explicitly. Therefore, because the data were self-reported, physicians may have attempted to place themselves in a positive light by characterizing their practice as being consistent with that recommended in the literature. However, in order to do this, they would at least need to be familiar with the literature on HRT.
In summary, our study shows that the prescribing practices of the Ontario physicians surveyed are consistent with recommendations on HRT use in the medical literature.
We thank the physicians who took the time to complete the questionnaire for this study. We also thank Ms. Donna Polyak for providing data entry.
Support for this work was provided by the Clinical Epidemiology Unit of the Sunnybrook Health Science Centre, North York, Ont., a contribution from Novartis Pharmaceuticals Canada Inc. and a fellowship (to Dr. Elinson) from the National Health Research and Development Programme. Dr. Cohen is the recipient of a Senior Scientist Award from the Medical Research Council of Canada. The investigators retained all rights to control entirely the methods, conclusions and means of publication of the study.
Competing interests: None declared.
Footnotes
-
This article has been peer reviewed.
Correspondence to: Dr. Lynn Elinson, Westat, 1650 Research Blvd., Rockville MD 20850, USA; [email protected] [Reprints will not be available from the authors.]
References
In this issue
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

