


Antimicrobial resistance is an increasing problem and challenge worldwide. Methicillin-resistant Staphylococcus aureus (MRSA) is the most commonly identified antimicrobial-resistant pathogen in areas of the world where these data are available. Rates of MRSA among clinical isolates of S. aureus vary from less than 1% in Norway and Sweden, 5%–10% in Canada, 25%–50% in the United States, to more than 50% in Hong Kong and Singapore.1 In a multinational survey of nosocomial pathogens, none of the clinical enterococcal isolates from South Africa, Egypt, Saudi Arabia or Lebanon were vancomycin-resistant enterococci. However, 7% of isolates from Germany and 16.7% of isolates from Switzerland and Greece were vancomycin-resistant enterococci.2 Resistance among these pathogens is much more prevalent among nosocomial infections than among community-acquired infections.3 The hypervirulent strain of Clostridium difficile, identified as a cause of outbreaks in North America, has been detected in an increasing number of European countries, affecting hospitals in 11 European Union member states and Switzerland.4
Four key hospital interventions — hand hygiene, environmental cleaning, barrier precautions and screening — are the cornerstones of infection control. In this article, we review the current knowledge and best practices in these areas.
Background
Epidemiological data show that MRSA, vancomycin-resistant enterococci and C. difficile are on the rise worldwide1–7 and that they have the potential to become important pathogens and endemic in Canada.8–10
Of particular concern in Canada are the outbreaks of C. difficile–associated disease with increased morbidity and mortality that have occurred in Quebec,8,11 the emergence of community-acquired MRSA9 and the increasing number of hospital-acquired MRSA infections.12 In a study conducted in 11 emergency departments in the United States in August 2004, 78% of S. aureus skin and soft-tissue infections were due to community-acquired MRSA.6 The public has become increasingly aware of the threat posed by “superbugs” and, understandably, expects that hospitals do better to prevent transmission to patients.13
Data from the Canadian Nosocomial Infection Surveillance Program show that, for every 1000 hospital admissions in 2007, there were 8.62 new patients with MRSA infection,14 and that, in 2005, there were 1.32 new patients with vancomycin-resistant enterococci per 1000 admissions.10 A 6-month survey from November 2004 to May 2005 identified 4.5 patients with C. difficile–associated disease for every 1000 admissions.15
Patients who have an infection (i.e., multiplication of an infectious agent in their tissues, resulting in subclinical or clinical illness) or colonization (i.e., presence of microorganisms without tissue invasion or injury) serve as reservoirs for these microorganisms. The risk factors for colonization include such factors as age, severity of illness and use of antibiotics (Box 1). The fact that patients may serve as a source of infection for fellow patients is supported by studies showing that the presence of greater numbers of concurrently infected patients in a ward (colonization pressure) and sharing a room with an infected patient are independent risk factors for acquiring C. difficile–associated disease, MRSA or vancomycin-resistant enterococci.16–19 Other studies have reported that the environment of patients with C. difficile, MRSA and vancomycin-resistant enterococci is frequently contaminated with these organisms, as are the hands, protective gowns and equipment used in the provision of care.19–25

The hospital provides a suitable environment for an infectious agent to come into contact with a susceptible host. Any intervention that successfully breaks just 1 link in the host–environment–agent chain will interrupt transmission. Below we describe 4 interventions that represent high priorities for action.
Interventions
Hand hygiene
Studies performed during the last decade have documented reductions in the rates of MRSA and vancomycin-resistant enterococci in hospitals that introduced alcohol-based, waterless hand antiseptics, usually in the context of a general campaign promoting hand hygiene as the cornerstone of safe patient care.26–29 Although these and other studies reported improved compliance with hand hygiene, at best compliance improved to 66% of opportunities for hand hygiene in 1 study27 and 48% in another.30 Sadly, in the study by Pittet and colleagues, physicians were least compliant with hand hygiene (performed in about 30% of hand-hygiene opportunities), and compliance did not improve during the course of the study.27 Although some studies have demonstrated more success with improving hand-hygiene compliance among physicians,31,32 the findings by Pittet and colleagues are consistent with other studies that have examined compliance with hand hygiene among different types of health care providers.33,34 Although important in hand hygiene, alcohol-based hand-hygiene products alone are insufficient to bring hand-hygiene compliance even close to 100%.31
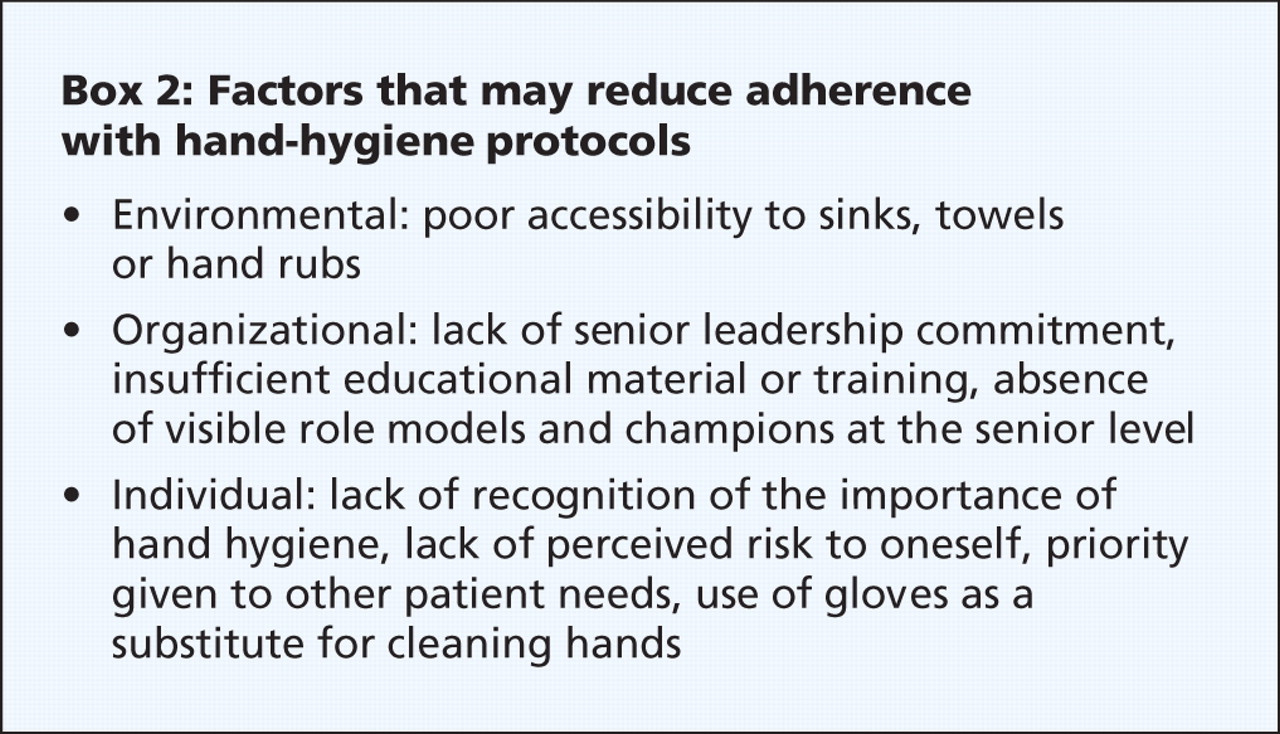
The predictors of physicians' adherence with hand hygiene were awareness of being observed, the belief of being a role model for other colleagues, a positive attitude toward hand hygiene after patient contact, and easy access to hand-rub solution. The risk factors for nonadherence were high workload, activities associated with a high risk of cross-transmission, and specialties such as surgery, anesthesiology, emergency medicine and intensive care medicine (Box 2).35

One approach that has received growing attention and some success among planners of programs that are focused on changing behaviour is social marketing. Social marketing incorporates commercial marketing technologies to influence voluntary behaviour, including not only the behaviour of the target audience but also of their immediate society (e.g., patients, other health care providers and visitors).36 Interventions, messaging and modes of communication strategically combine and integrate individual, organizational and environmental factors that affect compliance in such a way as to positively influence hand-hygiene behaviour. Initial evaluations of the social marketing approach have been positive in other areas of behaviour modification, but careful evaluation is crucial to ensure that marketing strategies for hand hygiene have long-term success in effecting change.37–39
Environmental cleaning
Next in importance to hand hygiene is the need to establish and maintain a clean and orderly health care environment (Table 1). MRSA, vancomycin-resistant enterococci and C. difficile persist in the environment and have been recovered from a number of commonly touched items such as keyboards, doorknobs, medical charts, bathtubs, toilets and furniture.20–23 There is debate as to whether the environment is responsible for the colonization of patients or whether soiled surfaces simply increase the likelihood of cross-transmission via contaminated hands.40,41 Cleaning has been associated with containment of outbreaks of C. difficile, vancomycin-resistant enterococci and MRSA.42 However, multiple interventions occurred during these events, and it is impossible to determine the contribution of cleaning as an individual measure.43 Common sense dictates that cleaning will never completely eliminate microorganisms from surfaces and that any disinfection is temporary at best. Regardless, an argument can be made to decrease the microbial burden through regular and thorough cleaning, particularly for shared clinical equipment, such as commodes, toilets and lifting equipment, or high-touch surfaces, such as keyboards.24,43
Table 1.
The efficacy of various disinfectants, particularly for C. difficile, has been the subject of debate, with different studies advocating or criticizing the use of bleach or hydrogen peroxide solutions in particular.44–46 What must not be forgotten in this debate is the importance of the mechanical action and thoroughness of the cleaning effort. Meticulous care must be taken to avoid cross-contamination of the environment via contaminated mop heads, cleaning solutions or cloths. The basic principles of keeping clutter to a minimum, cleaning from the top down and the use of fresh solutions in the correct concentration for adequate contact time are worth repeating. To do this properly, time and sufficient staff are required. The reflex to decrease the number of housekeeping staff to cut costs is short-sighted because it may be followed by an increase in more costly cross-transmission of hospital-associated microorganisms. Additionally, all health care workers need to understand that they have a responsibility for maintaining a clean environment and that this is not simply a “housekeeping” issue.
Barrier precautions
In Canada, the term “routine practice” refers to the infection prevention and control measures that are to be taken when providing care to all patients.47 In addition to hand hygiene, the tools used are gloves, gowns, masks and eye protection. As part of routine practice, gloves are used when there is anticipated exposure to a patient's blood, body fluids, mucous membranes, excretions, secretions, draining wounds or nonintact skin, and when handling items visibly soiled with blood, body fluids, secretions or excretions. Gowns, masks and eye protection are used to protect uncovered skin, clothing and mucous membranes from splashes or sprays of blood, body fluids, secretions and excretions. Under certain circumstances, when routine practice affords insufficient protection against the cross-transmission of microorganisms (to either health care workers or other patients), additional precautions such as “contact precautions” are required. The assumption is that patients or their environments, or both, are colonized and contaminated in the absence of blood, body fluids, excretions, secretions and visible soiling.
Contact precautions stipulate that gloves are to be worn when entering a patient's room or bed space and that a gown is to be worn for direct contact with a patient and his or her potentially, but not necessarily visibly, contaminated environment. A mask is required as part of “droplet precautions” to protect mucous membranes from contamination with infectious droplets. Placement of patients with antimicrobial-resistant organisms in private rooms or grouping patients harbouring the same bacteria is also recommended to reduce cross-transmission. The Public Health Agency of Canada notes that the evidence to support the use of contact precautions to prevent the cross-transmission of antimicrobial-resistant microorganisms is not strong.47
The use of contact precautions to prevent transmission of C. difficile, MRSA and vancomycin-resistant enterococci has been met with reservation for a number of reasons. Until recently, many hospitals in the United States have resisted adopting these measures because of incongruencies in national and international guidelines regarding recommendations for use of contact precautions,48,49 the lack of high-quality studies to support their implementation, and, in particular, a lack of resources to apply these interventions quickly, efficiently and consistently. The potential negative consequences of isolation, including social isolation, decreased examination of patients and poorer care, have been noted.50,51 Patients in isolation have decreased contact with health care workers, more preventable adverse events and greater dissatisfaction with their treatment,52 and they experience more depression and anxiety than patients not in isolation.53
Similar to studies that examine environmental cleaning as a measure to prevent cross-transmission of microorganisms, those that examine the role of barriers (e.g., gloves, gowns and masks) are frequently conducted in association with other interventions such as enhanced screening for carriers and housing patients in private rooms. The types of barriers applied also differ from study to study; some use gloves and gowns for room entry, while others use gloves alone for room entry and gowns only when there is direct contact with the patient. Some studies have been performed during a facility outbreak, whereas others have been performed in nonoutbreak situations. The relative effectiveness of individual interventions is thus difficult to assess. Despite this, there are a number of studies that point to a positive effect of contact precautions and private rooms in reducing the rates of colonization or infection with MRSA and vancomycin-resistant enterococci in both outbreak and nonoutbreak settings,52–61 although others have discounted the value of these interventions.62,63
Of particular note is the search and destroy approach for MRSA undertaken in the Netherlands.64 This strategy involves the preemptive quarantine in a single room of any patient previously admitted to hospital outside the Netherlands until 3 sets of cultures have been negative for MRSA. Personnel entering the room are required to wear a mask, cap, gown and gloves. Health care workers who have been in contact with a colonized patient are screened for MRSA and decolonized if they test positive. This search and destroy policy is credited for achieving and maintaining a very low rate (< 1%) of MRSA in the Netherlands.64–66 Similar low rates in western Australia have also been attributed to long-standing policies of rigorous screening and isolation.67
The literature is contradictory about the benefit of masks in the prevention of cross-transmission of S. aureus,49 apart from their role in preventing droplet transmission in the setting of a patient colonized with MRSA with respiratory symptoms.68 Vancomycin-resistant enterococci does not colonize the respiratory tract, and there is no role for masks in preventing cross-transmission.
The optimal precautions for each situation have not been conclusively identified, and this is likely to take a number of years. In the meantime, most Canadian acute care hospitals have taken an aggressive approach, with the majority of hospitals surveyed in 2002 using gowns and gloves for entry into patients' rooms.69
In terms of C. difficile–associated disease, a before–after study reported that the use of vinyl gloves was associated with reduced incidence of C. difficile in wards where gloves were supplied at the bedside and their use encouraged for providing care to patients with C. difficile.70 Given the degree of environmental contamination linked to C. difficile–associated disease, these patients should, at minimum, have their own dedicated toilet or commode until their symptoms have resolved, and there should be strict attention to cleaning.47
Screening
Ideally, routine practices would be sufficient to prevent person-to-person spread or cross-transmission of microorganisms. It is abundantly clear that this is not the case. If additional precautions are to be applied, it is imperative that the patients for whom these precautions are necessary be identified in a timely manner. This may be done by screening patients believed to be at risk for colonization with MRSA and vancomycin-resistant enterococci. Screening for vancomycin-resistant enterococci involves obtaining a rectal swab or stool sample for culture. Sites sampled for MRSA are more varied and are, in part, dependent on the culture methods, but may include the anterior nares, axillae, rectum, groins or perineum, and any open lesions.
In 1999, Papia and colleagues proposed that screening patients for MRSA was cost-effective based on modelling rates of infection, intervention effectiveness and costs.71 Many studies conducted in the United States and Europe have confirmed this observation and found that it also applies to screening patients for vancomycin-resistant enterococci.61,72–76 Relying on cultures from clinical specimens may miss up to 85% of patients colonized with MRSA.77 Colonized patients, in addition to those who are ill, represent a reservoir for transmission.78,79 Effective strategies should therefore include screening all patients who are at risk of colonization, by virtue of recent contact with a health care setting, although the nature of contact may vary from centre to centre.71,72,74
Although some patients may clear their colonization with MRSA and vancomycin-resistant enterococci, many remain colonized (persistently or intermittently) for many years.79 Most hospitals take a conservative approach and identify these patients as colonized for future admissions.69 Although studies are ongoing, the balance of evidence does not support routinely decolonizing patients with MRSA and vancomycin-resistant enterococci.79
Summary
Experience and evidence have taught us that the core components of infection prevention and control are consistent application of proper hand-hygiene measures, maintenance of a clean environment, use of barriers where appropriate, and prompt identification of patients at high risk of colonization with a transmissible microorganism. These components apply to all infections, whether or not the pathogen is known. Gaps in knowledge exist, such as a complete and integrated understanding of the determinants and facilitators for hand hygiene, identifying which barrier precautions offer the most benefit for the least risk, and predicting situations in which screening is most cost-effective.
-
Hand hygiene is the single most important measure for preventing the spread of infections.
-
Compliance with hand-hygiene measures is poor, especially among physicians.
-
Patient care environments may be the source of microorganisms, and should be kept clean and tidy.
-
Barrier precautions play a role in preventing cross-transmission of microorganisms in acute care facilities.
-
Screening of patients at high risk for colonization with methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci may be cost-effective if coupled with barrier precautions.
Key points
-
Nicolle L, Conly JM, MacDonald N. Embracing ecology to limit antimicrobial resistance. CMAJ 2009;180:371-2.
-
Mulvey MR, Simor AE. Antimicrobial resistance in hospitals: How concerned should we be? CMAJ 2009;180:408-15.
-
Patrick DM, Hutchinson J. Antibiotic use and population ecology: How you can reduce your “resistance footprint.” CMAJ 2009;180:416-21.
Articles to date in this series
Footnotes
-
This article has been peer reviewed.
Contributors: Lynn Johnston and Elizabeth Bryce contributed equally to identifying and reviewing the literature, and writing the first and subsequent drafts of the manuscript. Both authors approved the final version submitted for publication.
Competing interests: None declared.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.
- 18.
- 19.↵
- 20.↵
- 21.
- 22.
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

