


A previously healthy 3-year-old boy was brought to hospital by his mother, who was concerned that he had ingested several small, spherical magnets earlier that day. The only symptom noted by his mother was increased drooling. Physical examination was unremarkable and revealed a child in no distress. Abdominal radiographs showed 2 small, round radiopacities in the right lower quadrant and one in the epigastrium (Figure 1A) consistent with the description of the magnets. No free air or other signs of perforation were visible. After consultation with the nearby children’s hospital, the child was transferred for a gastroenterology opinion and possible endoscopy.
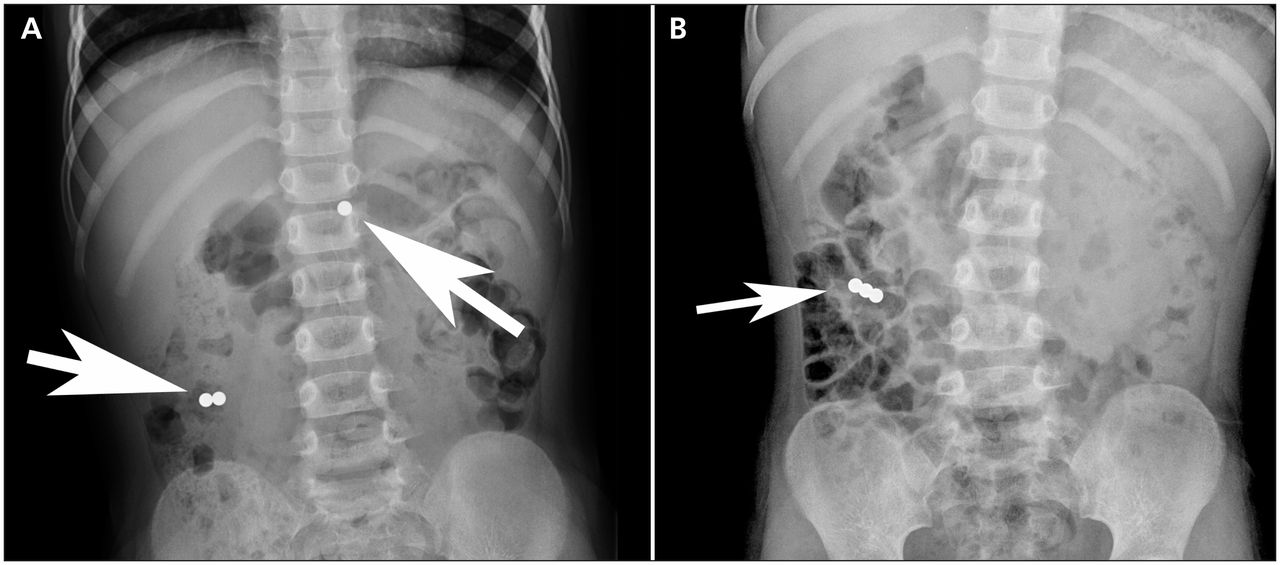
Radiographs (anteroposterior view), showing (A) magnets in the epigastrium and right lower abdominal quadrant of a 3-year-old boy and (B) the magnets 2 days later in the right lower quadrant.
Repeat imaging at the children’s hospital revealed no change from the previous radiographs. The gastroenterology service performed an esophagogastroduodenoscopy to the proximal jejunum in an attempt to remove the magnet. However, the magnet had migrated beyond the reach of the endoscope. Given the child’s unchanged clinical status of stable vital signs, no fever, no lethargy and no abdominal pain, he was discharged home. His parents were instructed to monitor his stool for passage of the magnets and educated on the signs and symptoms of intestinal perforation.
After 2 days, the child was brought back to the children’s hospital because he had not passed any magnets and now had abdominal pain. Radiographs showed that all 3 magnets had come together in the right lower quadrant (Figure 1B). His vital signs were normal. Given the increasing potential for bowel perforation, the child was admitted to hospital for monitoring, serial radiographs and administration of a laxative (polyethylene glycol 3350). No blood work was deemed necessary.
The following day, despite 2 watery bowel movements, the child still did not pass the magnets. Later that day, he had a fever (38.7°C) and tachycardia (138 beats/min). Radiographs showed no changes in the position of the magnets and no free air. After an in-depth discussion of the risks and benefits of operative management with the parents, laparoscopy was performed. Three neodymium magnets, each 5 mm in diameter, were found adhering to each other, having eroded through 2 loops of ileum. They were removed via laparascopic-assisted enterotomy, and primary repair of the perforations was performed through the umbilical incision. There were no postoperative complications, and the child was discharged home 4 days later.
Discussion
Magnets have evolved tremendously in the past 25 years. Neodymium–iron–boron magnets (a type of rare-earth magnet) were created in the early 1980s and are 10–20 times stronger than traditional ferrite magnets. Widespread licensing of patents, decreasing prices and improved manufacturing technology in the early 2000s has fuelled widespread release of magnet-based consumer products such as desk toys, children’s construction sets and jewellery. Swallowing a single magnet is generally innocuous, much like swallowing any other inert foreign body.1 However, multiple magnets, especially when swallowed at different times, can attract each other through loops of the gastrointestinal tract. The force created through the bowel or stomach wall may result in pressure necrosis and eventual perforation.
Epidemiology
Ingestion of magnets has traditionally been described as rare.2 However, a recent review3 found that only 3 of 44 case reports were published before 2002. In the last year alone, our general surgery service was asked to see 13 children who had swallowed magnets; 4 required operative management and a prolonged hospital stay.
Our institutional experience reflects both Canadian and American surveillance data. The US Centers for Disease Control and Prevention issued its first warning about this new generation of magnets in 2006.4 In a review of surveillance data in Canada from 1993 to 2007, the Public Health Agency of Canada reported that 328 children under 14 years old were brought to an emergency department because of an injury associated with magnets; just over half (178 [54.5%]) had swallowed the magnets.5 The agency noted that the number of presentations had increased sharply in the last decade reviewed, after a small and stable number of reports during the 1990s. In a 2012 survey, members of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition reported 480 cases of high-powered magnet ingestions in the previous 10 years, 204 of which were in the previous 12 months.6
Presentation
Historically, ingestion of magnets was treated like any other foreign body, with only slightly more cause for caution. Traditional ferrite magnets were large and magnetically weak, unlikely to damage the gastrointestinal tract. With new neodymium–iron–boron technology, magnets have become smaller, stronger and more prevalent. Patients usually present either with known or suspected ingestion, as in our patient, or with vomiting, abdominal pain and fever. These non-specific signs and symptoms, common in the pediatric population, can lead to substantial delays in diagnosis. In response to this challenge, the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition published an algorithm addressing the complexity of managing ingested magnets (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121847/-/DC1).7 It stresses the importance of close clinical monitoring; the increased use of plain radiographic imaging; and the collaboration of primary care physicians, gastroenterologists and surgeons.
Management
Generally, the management begins once plain radiographs have confirmed the presence of a foreign body consistent in shape and size with a magnet. Single magnets are of least concern and generally require only close monitoring, prevention of further ingestions, parental education and the avoidance of extrinsic metallic or magnetic objects.7
When multiple foreign bodies are seen, management is more complicated. If, on serial imaging, the magnets appear to be bound together and mobile, they should be expected to pass together as a unit. If they are bound together but are immobile, it can be inferred that they are anchoring each other through the bowel wall, and a perforation is likely. If multiple individual magnets or groups of magnets are seen, there is a risk that they will link and anchor to each other across loops of bowel.
If possible, magnet retrieval with endoscopy is recommended.7 If the patient is asymptomatic and serial radiographs show progression of the magnets in the gastrointestinal tract, discharge home with close follow-up and detailed instructions to parents can be considered.7 As medical management, polyethylene glycol 3350 can be used to aid passage. Should these methods fail, surgical removal is required.7
Awareness and prevention
Primary prevention is the best way to avoid the morbidity associated with magnet ingestion. Although health care providers can play an important role in disseminating information on the risks of magnet ingestion, further targeted campaigns are needed to inform parents of the risks. Small warning labels on magnet-based products have been insufficient. Media exposure on the topic and information in primary care offices are needed. The 18-month well-baby visit may be an appropriate time to discuss magnet safety in the context of safe toys.
Making all health care providers aware of this danger is of paramount importance. In 2007, the Canadian Paediatric Surveillance Program sent a one-time survey question on magnetic toys to 2442 practising pediatricians. Only 61% of the respondents were aware of the health hazards related to these toys.8
Front-line providers need to be aware of the special circumstances involving developmentally delayed children and children with autism or attention-deficit/hyperactivity disorder, because these children are more prone to magnet ingestions and require a higher degree of suspicion to be properly identified.9 One group has advocated that all pediatric patients undergo ferromagnetic screening before undergoing magnetic resonance imaging (MRI), in light of a case report of a child who had surreptitiously ingested a magnet and in whom a gastrointestinal perforation developed following MRI of his neck for an unrelated health concern.10
At a regulatory level, Health Canada and the Consumer Products Safety Commission in the United States have been working to keep high-powered magnets out of the hands of children. Several high-profile toy recalls and mandates that companies manufacturing magnetic desk toys make it clear they are not intended for children appear to have been insufficient. In 2012, the US Consumer Products Safety Commission began developing a new federal standard for small, high-powered magnet sets.11 Australian and New Zealand authorities have also taken action by issuing a ban on small, high-powered magnets from children’s toys, construction kits and jewellery.12,13 Such regulatory interventions are the first step toward preventing magnet ingestions, but they do nothing for products already sold, or magnets in products not covered by the bans.
Conclusion
Modern magnet technology has transformed what was once an esoteric type of foreign-body ingestion into a common and lethal threat. Despite efforts in many countries, high-powered magnets are here to stay. Through primary prevention, effective recognition of the problem and prompt, appropriate management with multidisciplinary collaboration, the risks associated with magnet ingestions can be mitigated.
Key points-
Gastrointestinal perforation from the ingestion of multiple magnets is becoming a more frequent and life-threatening problem.
-
This change is being driven by a recent surge in the availability of more powerful rare-earth magnets.
-
Management should include liberal use of radiographs, and collaboration between primary care and emergency physicians, gastroenterologists and general surgeons.
-
Regulatory changes, health care provider awareness and parent education about magnet safety are important components in mitigating risks of magnet ingestion.
Acknowledgements
The authors thank Dr. Jacob Langer for providing them with intraoperative photographs. The authors also thank the patient’s family for generously providing consent to report their child’s case.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
-
Contributors: All of the authors contributed substantially to the writing and revision of the manuscript and approved the final version submitted for publication.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

