


Abstract
BACKGROUND: Ethnicity may be associated with important aspects of end-of-life care, such as what treatments are received, access to palliative care and where people die. However, most studies have focused on end-of-life care of white, Hispanic and black patients. We sought to compare end-of-life care delivered to people of Chinese and South Asian ethnicity with that delivered to others from the general population, in Ontario, Canada.
METHODS: In this population-based cohort study, we included all people who died in Ontario, Canada, between Apr. 1, 2004, and Mar. 31, 2015. People were identified as having Chinese or South Asian ethnicity on the basis of a validated surname algorithm. We used modified Poisson regression analyses to assess location of death and care received in the last 6 months of life.
RESULTS: We analyzed 967 339 decedents, including 18 959 (2.0%) of Chinese and 11 406 (1.2%) of South Asian ethnicity. Chinese (13.6%) and South Asian (18.5%) decedents were more likely than decedents from the general population (10.1%) to die in the intensive care unit (ICU). The adjusted relative risk of dying in intensive care was 1.21 (95% confidence interval [CI] 1.15 to 1.27) for Chinese and 1.25 (95% CI 1.20 to 1.30) for South Asian decedents. In their last 6 months of life, decedents of Chinese and South Asian ethnicity experienced significantly more ICU admission, hospital admission, mechanical ventilation, dialysis, percutaneous feeding tube placement, tracheostomy and cardiopulmonary resuscitation than the general population.
INTERPRETATION: Decedents of Chinese and South Asian ethnicity in Ontario were more likely than decedents from the general population to receive aggressive care and to die in an ICU. These findings may be due to communication difficulties between patients and clinicians, differences in preferences about end-of-life care or differences in access to palliative care services.
Culturally appropriate, patient-focused end-of-life care is an essential component of health care. Despite a preference to die at home, most Canadians die in hospitals and many receive end-of-life care in intensive care units (ICUs).1–3 Multiple factors contribute to this discrepancy, including uncertainty about the imminence of death, challenges in communication between health care teams and patients and families, poor health literacy and lack of access to palliative care resources.3–7 These factors may be more pronounced among people from minority ethnic groups. Differences in preferences for intervention at the end of life among ethnic groups may also influence care; the research showing a preference for dying at home included mostly white Canadians.1
People of Chinese and South Asian ethnicity are the most rapidly growing ethnic groups in Canada, yet little is known about their end-of-life care.8,9 Comparative studies from the United States have focused on black and Hispanic Americans8–13 and suggest that minority ethnicity is associated with lower family-rated quality of end-of-life care,14 increased use of life-support technologies, 13 and decreased use of advanced directives or hospice.6,12,15–17 Qualitative research describing end-of-life care for people of Chinese or South Asian ethnicities in international settings shows some common themes, including reluctance to share terminal diagnoses, emphasis on collective as opposed to individual decision-making, and attenuation of differences with acculturation. 6,18,19 For people of Chinese ethnicity, research highlights the influence of Confucian philosophy and the role of children in decisions regarding elderly parents.20–23 For people of South Asian ethnicity, research emphasizes notions of karma, ambivalence toward the cultural appropriateness of hospices or sedating analgesic medications, and the influence of common South Asian religions including Islam, Buddhism, Sikhism or Hinduism.24–30
In 2011, Ontario had a population of 12 851 821, of whom the 2 largest ethnic minority groups were South Asian (833 085, 6.5%) and Chinese (531 635, 4.1%).31 Previous research identified that people in Ontario who were born in South Asia or East Asia experienced end-of-life care that was different from that experienced by long-standing residents, but this analysis did not investigate patient ethnicity.32 We conducted this population-based analysis to describe end-of-life care delivered to people of Chinese and South Asian ethnicity compared with that delivered to others from the general population.
Methods
Study design, setting and data sources
We conducted a retrospective decedent cohort study analyzing patients who died in Ontario, Canada, between 2004 and 2015. Data regarding immigration status were obtained using the Permanent Resident Database maintained by Immigration, Refugees and Citizenship Canada.32 Identification of health care use before death was obtained using health administrative databases that were linked at the individual level: Registered Persons Database containing vital statistics on all people issued a provincial health card, Ontario Health Insurance Plan, Office of the Registrar General for Deaths, Discharge Abstract Database and National Ambulatory Care Reporting System.33,34 These databases contain comprehensive coverage of care provided in hospitals.35
Study cohort
All individuals who died in Ontario between Apr. 1, 2004, and Mar. 31, 2015, were eligible, excluding those enrolled in Ontario’s publicly funded health insurance plan for less than 6 months. People with missing baseline data (< 1%) were included only in unadjusted analyses.
Ethnicity was identified through a validated algorithm using surnames to identify patients of Chinese ethnicity (sensitivity 80.2%, specificity 99.7%) and South Asian ethnicity (sensitivity 50.4%, specificity 99.7%).36 This algorithm has been used to investigate multiple clinical questions in Ontario administrative health data.37–40 All decedents not identified as being of either Chinese or South Asian ethnicity were classified as being from the general population.
Patient characteristics included age, sex, socioeconomic position, place of residence at time of death, and cause of death. Health services data included palliative care physician visits, ICU admissions, hospital admissions and procedures during the final 6 months of life. The databases did not contain information on cardiopulmonary resuscitation (CPR) preferences or goals of care.
Decedents were classified as recently immigrated (since 1985) or long-standing resident (all others). For recently immigrated decedents, information obtained at the time of immigration application was available, including immigration class (economic, family, refugee and other), education level, language ability and country of birth.
Outcomes
The primary outcome described end-of-life care by location of death: ICU, acute care hospital, long-term-care facility (or nursing home), home or other (including hospice). The results are expressed as relative risks (RRs), comparing the proportions of decedents of Chinese or South Asian ethnicity with proportions of decedents from the general population who experienced a given outcome.
Secondary outcomes assessed interventions received in the last 6 months of life, including palliative care, hospital admission, ICU admission, mechanical ventilation, dialysis, percutaneous feeding tube, tracheostomy or CPR.
A decedent was classified as having received palliative care if there were administrative codes for palliative care visits in outpatient, inpatient, long-term care or complex continuing care settings (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.190655/-/DC1).41 The data included home care services provided to patients given an “end-of-life” designation by their physicians, but did not include home care services provided to patients without such a designation or services paid for out of pocket by patients or families.41
Statistical analysis
We assessed the association between ethnicity and end-of-life care outcomes using modified Poisson regression to estimate RRs.42 Outcomes included location of death (ICU, acute care hospital, long-term-care facility, home or other, including hospice) and care received in the last 6 months (hospital admission, ICU admission, mechanical ventilation, dialysis, percutaneous feeding tube placement, tracheostomy, CPR and palliative care). Patient covariates included age, sex, income quintile, urban or rural residence, cause of death and immigration status. The analysis used generalized estimating equations with an exchangeable correlation structure to account for geographic clustering.43
Recently immigrated decedents were separately analyzed with additional covariates unique to immigrated decedents, to investigate how an ethnicity covariate affected previously observed differences in end-of-life care by region of birth for recently immigrated decedents.32
We performed post-hoc interaction analyses of ethnicity and immigration status, and ethnicity and age group. If modified Poisson regression models did not converge, we used logistic regression. Two-sided p values less than 0.05 were considered significant, with no adjustment for multiple comparisons. We used SAS Enterprise Guide 6.1 and R 3.5 software.
Ethics approval
This study was approved by ICES, a prescribed entity allowing for use of patient information in approved research projects without patient consent.
Results
Demographic and clinical characteristics
We included 967 339 decedents, of whom 18 959 (2.0%) were of Chinese ethnicity and 11 406 (1.2%) were of South Asian ethnicity according to the surname algorithm. The median age at death was 80 (interquartile range 68–87) years, with cardiovascular causes (24.8%) the most common category of causes of death (Appendix 1). Compared with decedents from the general population, decedents of Chinese and South Asian ethnicity were less wealthy and more likely to live in an urban area (Table 1). The proportion of decedents who had immigrated to Canada since 1985 was higher among the decedents of Chinese (39.7%) and South Asian (49.5%) ethnicity than among decedents from the general population (3.7%).
Baseline characteristics of decedents from the general population and of Chinese and South Asian ethnicity in Ontario, Canada, between 2004 and 2015
End-of-life care
Of the 967 339 decedents, 99 783 (10.3%) died in intensive care. Compared with decedents from the general population, a higher proportion of decedents of Chinese (13.6% v. 10.1%, difference 3.4%, 95% confidence interval [CI] 3.0% to 3.9%) and South Asian ethnicity (18.5% v. 10.1%, difference 8.3%, 95% CI 7.6% to 9.0%) died in intensive care (Table 2 and Table 3). This increase persisted after adjustment for differences in age, sex, income, geography, cause of death and immigration status. The adjusted RR of dying in intensive care for decedents of Chinese ethnicity was 1.21 (95% CI 1.15 to 1.27) and for decedents of South Asian ethnicity was 1.25 (95% CI 1.20 to 1.30).
End-of-life care delivered to people of Chinese ethnicity compared with that delivered to others from the general population in Ontario, Canada, between 2004 and 2015
End-of-life care delivered to people of South Asian ethnicity compared with that delivered to others from the general population in Ontario, Canada, between 2004 and 2015
In the last 6 months of life, compared with decedents from the general population, decedents of Chinese and South Asian ethnicity experienced more ICU admission, hospital admission, mechanical ventilation, dialysis, percutaneous feeding tube placement, tracheostomy and CPR (Figure 1). Decedents of Chinese ethnicity had more, and decedents of South Asian had fewer, interactions with palliative care clinicians than decedents from the general population (Figure 1).
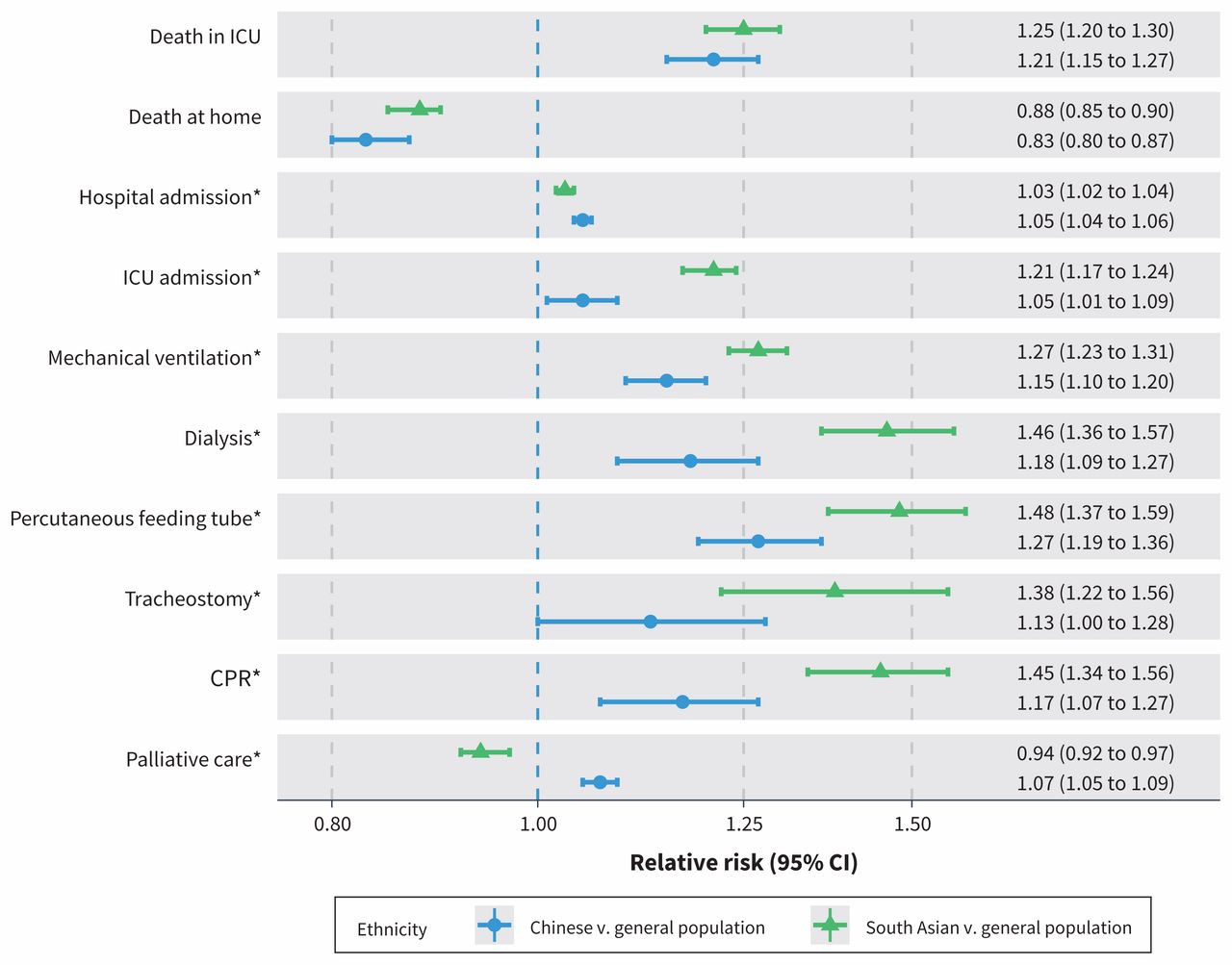
Forest plot showing the ratio of the proportions of decedents from each ethnicity experiencing each of the major study outcomes. Each comparison shows the relative risk (RR) of experiencing the outcome among Ontario decedents of either Chinese or South Asian ethnicity compared with the Ontario decedent general population. Each RR is derived from a modified Poisson regression model with generalized estimating equations incorporating age, sex, geography, socioeconomic position, cause of death and immigration status. Relative risks greater than 1 correspond to an increased RR of the outcome among Ontarians of Chinese or South Asian ethnicity. Note: CI = confidence interval, CPR = cardiopulmonary resuscitation, ICU = intensive care unit. *Interventions received in final 6 months of life.
Recently immigrated population subgroup
Our analysis included a subgroup of 47 553 recently immigrated people, of whom 7527 (15.8%) were of Chinese ethnicity and 5646 (11.9%) were of South Asian ethnicity (Appendix 1, Supplemental Table E1). Among decedents of Chinese ethnicity, there was an increase in the unadjusted RR of dying in intensive care when we compared recent immigrants with long-standing residents (14.4% v. 13.1%, difference 1.3%, 95% CI 0.3% to 2.3%). Among decedents of South Asian ethnicity, for the same comparison, there was no difference (18.5% v. 18.5%, difference 0.0%, 95% CI −1.4% to 1.4%). Among recently immigrated decedents, the adjusted RR of dying in intensive care for those of Chinese ethnicity compared with the general population was 1.08 (95% CI 0.97 to 1.20), and for those of South Asian ethnicity compared with the general population it was 0.93 (95% CI 0.86 to 0.99). This model included the same covariates as the base model as well as covariates unique to the recently immigrated decedent cohort (landing date, region of birth, language ability and education level on arrival, immigration type and years in Ontario at death).
Sensitivity analyses
Because the surname algorithms favour specificity over sensitivity, many decedents who identified as being of Chinese or South Asian ethnicity were classified as decedents from the general population. We estimated 4681 misclassified Chinese decedents and 11 225 misclassified South Asian decedents on the basis of test sensitivities and calculated that even if every decedent of Chinese ethnicity misclassified as being from the general population was not in the ICU at death, the unadjusted result would still retain significance (Appendix 1, Supplemental Figure E1). Similarly, the proportion of decedents of South Asian ethnicity misclassified as being from the general population who died in the ICU would have to be 3.2% or less (as opposed to the 19% proportion observed in correctly classified decedents) for the unadjusted differences to become not significant (Appendix 1, Supplemental Figure E2).
The interaction analysis of recent immigration and ethnicity showed greater differences in location of death among decedents who were long-standing residents relative to those who recently immigrated (Figure 2). The interaction analysis of age and ethnicity suggests increasing differences in location of death at ages greater than 80 years when comparing decedents of Chinese or South Asian ethnicity and decedents from the general population (Figure 2).

Forest plot showing the coefficients of the 2 interaction analyses (age by ethnicity and immigration status by ethnicity) with respect to the outcome of death in the intensive care unit (ICU) compared with all other locations. Each row shows the relative risk (RR) of being in the ICU at the time of death for decedents within the described subgroup comparing Ontario decedents of either Chinese or South Asian ethnicity with Ontario decedents from the general population. Each coefficient is derived from a regression model with generalized estimating equations incorporating age, sex, geography, socioeconomic position, cause of death and immigration status. Note: CI = confidence interval. *Coefficients for the interaction between immigration status and ethnicity are RRs from a modified Poisson regression model, and coefficients for the interaction between age and ethnicity are odds ratios from a logistic regression model owing to convergence difficulties with a modified Poisson model. Relative risks greater than 1 correspond to an increased RR of being in intensive care at death among Ontarians of Chinese or South Asian ethnicity.
Interpretation
Among decedents in Ontario, those of Chinese or South Asian ethnicity were more likely to receive aggressive end-of-life care and to die in intensive care than those from the general population. Differences in end-of-life care between cohorts persisted despite adjustment for age, sex, cause of death, socioeconomic position, urban versus rural geography, and immigration status.
The finding of more aggressive end-of-life care among decedents of Chinese or South Asian ethnicity is similar to the findings of other large-scale quantitative analyses assessing end-of-life care for people from ethnic minorities in North America such as Hispanic or black people.16,44,45 Although each ethnic group has multiple unique underlying contributors to these findings, some factors such as provider–patient ethnicity discordance, decreased socioeconomic resources and discrimination may be common to different minority ethnicities.5,46,47
We found contrasting results with respect to receipt of palliative care in the final 6 months of life, with decedents of South Asian ethnicity less likely, and decedents of Chinese ethnicity more likely, to receive palliative care relative to decedents from the general population. The results of qualitative research are conflicting regarding the attitudes toward and use of advanced care planning among people from East Asia, and further research is needed to better understand this finding.41,48,49
This study adds to the previously described association between immigration status and end-of-life care by showing that both recent immigration status and Chinese or South Asian ethnicity are independently associated with more aggressive end-of-life care.32 The previously identified association between recent immigration and more aggressive end-of-life care persisted even after adjustment for ethnicity. However, the interaction analyses emphasized that the largest differences in end-of-life care by ethnicity were seen in decedents who were long-standing residents. It is not possible to fully separate immigration and ethnicity in this analysis, because there were no data on birthplaces of long-standing residents, and many decedents of Chinese and South Asian ethnicity classified as long-standing residents may have immigrated to Canada before 1985.36
The observed variation in end-of-life care by ethnicity has multiple potential explanations, including patient preferences, health literacy, communication barriers, cultural differences, clinician behaviour, use of advanced directives, and differences in service accessibility.46 Differences in patient and family preferences may relate to religious and cultural beliefs, practices regarding death, notions of filial responsibility, or a preference for family-centred as opposed to individual decision-making. 18,19,21–24,26–28,41,43 Previous research documented an association between minority ethnicity and decreased knowledge of advanced care planning.12,50 Communication difficulties may exist between patients of Chinese and South Asian ethnicity and health care professionals because of differences in languages spoken, culture, beliefs about end-of-life care and communication styles, which may manifest as cultural insensitivity and lead to a lack of trust.3,28–30,51–54 Some clinical settings may have fewer health care professionals of minority-ethnicity backgrounds.55 Lastly, people of Chinese or South Asian ethnicity may have fewer financial or social resources to help them pay for or provide non–publicly funded outpatient end-of-life care.3,6,24
Limitations
This observational study has several limitations. The surname algorithm to identify patient ethnicity is optimized for specificity but has only moderate sensitivity. Although the algorithm was derived for use in the databases employed in this study, it has been validated only once in that database.36 We attempted to quantify the potential impact of misclassified decedents in our sensitivity analyses. The introduction of confounding as a result of the surname algorithm is possible. For example, the South Asian surname list includes more names of Sikh, Hindu or Sri Lankan backgrounds and fewer names of Christian or Muslim backgrounds.36 Differences in comorbidities or cause of death not captured by the category of cause of death are another potential source of unmeasured confounding. The adjustment for geography is also fallible because some people may be able to access relatively scarce resources, such as palliative care, regardless of geographic location.56 The findings describe care in Ontario and may have limited generalizability to other Canadian provinces or territories, or other countries. This research is further limited by the lack of qualitative data on medical decision-making, the attitudes toward treatment and the experience of end-of-life care for people of Chinese or South Asian ethnicities. Lastly, we had no data about the language or health literacy, religion, or goals of care for patients or families.
Conclusion
Among decedents in Ontario, people of Chinese and South Asian ethnicity were more likely than people from the general population to receive aggressive care and to die in an ICU. These differences may relate to preferences of patients or their substitute decision-makers, health literacy, decision-making or communication with health care professionals, or access to care.
Acknowledgements
The authors thank Dr. Baiju Shah for thoughtful feedback and advice regarding the manuscript and use of the surname-based algorithm. The authors also thank Immigration, Refugees and Citizenship Canada for providing access to the Permanent Resident Database of landed immigrants.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Christopher Yarnell contributed to the concept, study design, literature review, data analysis and data interpretation. Longdi Fu contributed to the study design and data analysis. Michael Bonares contributed to the data interpretation. Ayah Nayfeh contributed to the study design, concept and data interpretation. Robert Fowler contributed to the concept, study design, literature review, data analysis and data interpretation. Christopher Yarnell contributed to the writing, table and figure creation, appendix creation and critical review. Longdi Fu and Michael Bonares contributed to the critical review. Ayah Nayfeh contributed to the critical review and writing. Robert Fowler contributed to the writing, table and figure creation, funding and critical review. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: The study was funded by the Canadian Institutes of Health Research (CIHR), Heart and Stroke Foundation of Ontario, the Canadian Frailty Network Centre of Excellence and the University of Toronto Integrating Challenge Fund. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; nor in the decision to submit the manuscript for publication.
Disclaimers: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES, Immigration, Refugees and Citizenship Canada or the Ontario MOHLTC is intended or should be inferred.
Parts of this report are based on Ontario Registrar General information on deaths, the original source of which is ServiceOntario. The views expressed therein are those of the authors and do not necessarily reflect those of the Ontario Registrar General or Ministry of Government and Consumer Services.
Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed in the material are those of the authors, and not necessarily those of CIHI.
These data sets were linked using unique encoded identifiers and analyzed at ICES.
- Accepted January 10, 2020.
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Palliative care symptoms and problems in a culturally and linguistically diverse population: large retrospective cohort study
- Association between patient race/ethnicity and invasive ventilation in hypoxemic respiratory failure
- Discussing prognosis and what matters most for people with serious illness
- Ethnicity and "aggressive" end-of-life care
More in this TOC Section
Similar Articles
Collections

