


Idiopathic intracranial hypertension primarily affects young obese women
More than 93% of people with idiopathic intracranial hypertension (previously called pseudotumour cerebri and benign intracranial hypertension) are obese. The annual incidence of the disease is highest among young obese women, at an estimated 20 per 100 000.1 The median age at onset is 34 years.1 A higher body mass index and a higher percentage of weight gain in the past year are associated with increased risk.2 Medications can also cause elevated intracranial pressure (see point 5).
Diagnosis is based on clinical features, an intracranial pressure greater than 250 mm H2O and no culprit lesion on neuroimaging
Daily headaches, which may be incapacitating, and reduced vision are the hallmark symptoms. (The diagnostic criteria for idiopathic intracranial hypertension are listed in Appendix 1, at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110072/-/DC1.) The vision changes are secondary to swelling of the optic nerve due to raised intracranial pressure (papilledema) (Figure 1), which is evident clinically in up to 95% of patients with idiopathic intracranial hypertension.3 Transient visual obscuration — vision loss or “dimming” lasting seconds — is the most commonvisual symptom. Visual acuity is often impaired less than visual field in these patients. Horizontal diplopia from abducens nerve paresis may also occur. Pulsatile tinnitus, present in 60% of patients, was shown to be the most specific symptom in a large case–control study.4
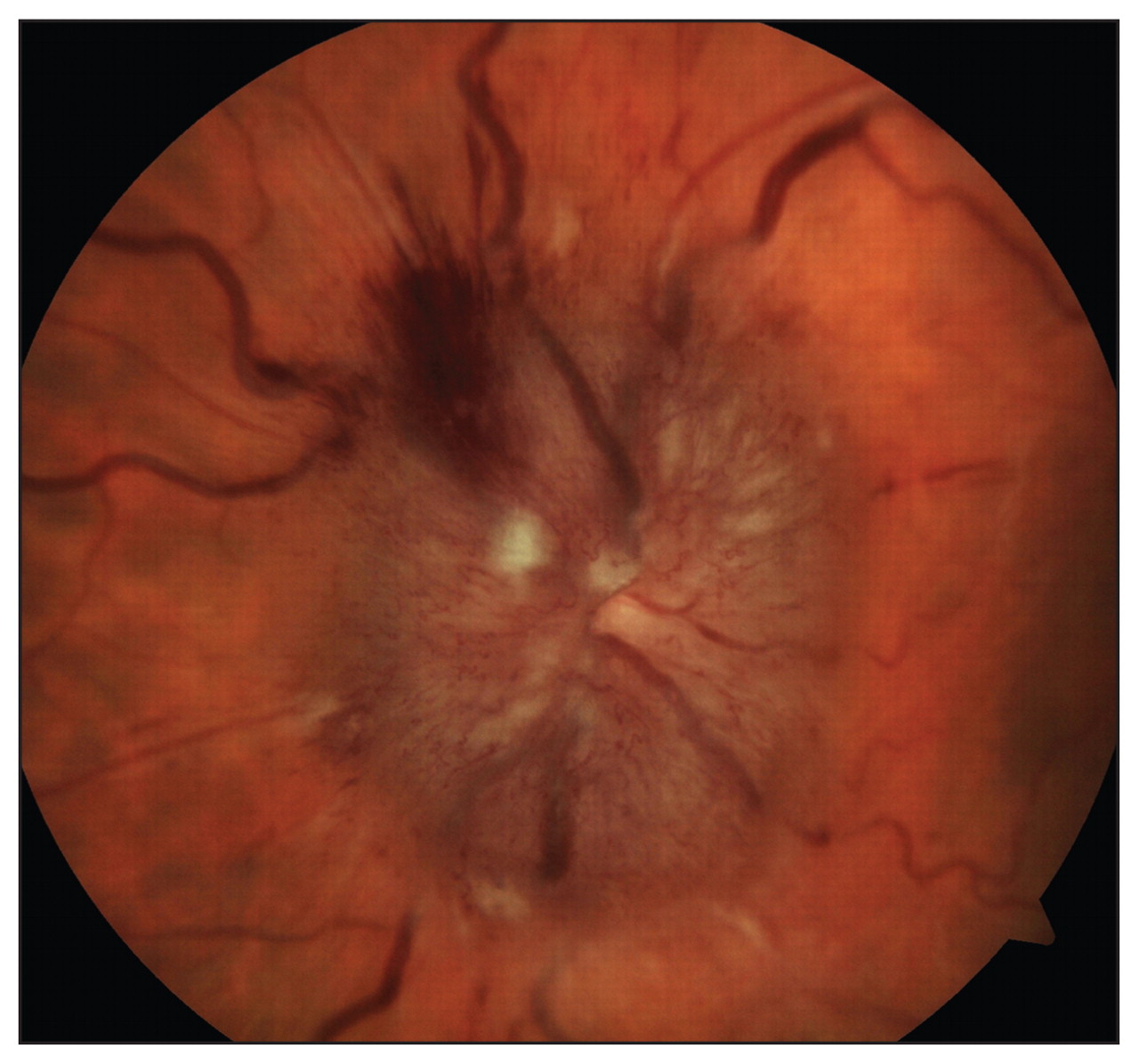
Papilledema in a young obese woman with idiopathic intracranial hypertension. The degree of papilledema does not correlate with the intracranial pressure or the degree of visual dysfunction.
Magnetic resonance venography can rule out important alternate diagnoses
In addition to ruling out structural causes of increased intracranial pressure, most importantly neoplasms, magnetic resonance venography can rule out cerebral venous sinus thrombosis, which is the main differential diagnosis in young women, particularly those taking oral contraceptives.5
Management strategies lack robust evidence, but weight loss is the cornerstone
Management strategies have gained acceptance based on clinical success over many years, but large prospective trials are lacking.6 A strategy of weight loss, restricted sodium intake and acetazolamide (250 mg four times daily) has become common practice. For progressive vision loss, insertion of a cerebrospinal fluid shunt, and in some centres fenestration of the optic nerve sheath, may be offered.6
Medications associated with increased intracranial pressure should be stopped
Tetracycline and related compounds, vitamin A and analogs, steroids and lithium are among the agents that have been associated with increased intracranial pressure.5
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Jump to section
- Article
- Idiopathic intracranial hypertension primarily affects young obese women
- Diagnosis is based on clinical features, an intracranial pressure greater than 250 mm H2O and no culprit lesion on neuroimaging
- Magnetic resonance venography can rule out important alternate diagnoses
- Management strategies lack robust evidence, but weight loss is the cornerstone
- Medications associated with increased intracranial pressure should be stopped
- Footnotes
- References
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

