


Abstract
Background: The increasing incidence of injuries related to playing ice hockey is an important public health issue. We conducted a systematic review to evaluate the effectiveness of interventions designed to reduce injuries related to aggressive acts in ice hockey.
Methods: We identified relevant articles by searching electronic databases from their inception through July 2012, by using Internet search engines, and by manually searching sports medicine journals, the book series Safety in Ice Hockey and reference lists of included articles. We included studies that evaluated interventions to reduce aggression-related injuries and reported ratings of aggressive behaviour or rates of penalties or injuries.
Results: We identified 18 eligible studies. Most involved players in minor hockey leagues. Of 13 studies that evaluated changes in mandatory rules intended to lessen aggression (most commonly the restriction of body-checking), 11 observed a reduction in penalty or injury rates associated with rule changes, and 9 of these showed a statistically significant decrease. The mean number of penalties decreased by 1.2–5.9 per game, and injury rates decreased 3- to 12-fold. All 3 studies of educational interventions showed a reduction in penalty rates, but they were not powered or designed to show a change in injury rates. In 2 studies of cognitive behavioural interventions, reductions in aggressive behaviours were observed.
Interpretation: Changes to mandatory rules were associated with reductions in penalties for aggressive acts and in injuries related to aggression among ice hockey players. Effects of educational and cognitive behavioural interventions on injury rates are less clear. Well-designed studies of multifaceted strategies that combine such approaches are required.
Over the last 15 years, the incidence of brain and spinal cord injuries among ice hockey players has increased.1 A recent study involving players in junior leagues found that, in the 2009/10 hockey season, the incidence of game-related concussions was 7 times higher than the highest rate previously reported in 1998/99.2 Brain injuries frequently result from aggressive bodychecking3 and account for 15% of injuries among players 9–16 years of age.4,5 In a study of a community-based hockey program involving boys aged 9–15 years, hostile aggressive acts, which have an intention to do harm,6 were the primary cause of injury in one-third of games in which an injury resulted.7 Among high school students in Minnesota who played varsity ice hockey, those who played to relieve aggression were 4 times more likely than other players to experience a concussion.8 These findings highlight the association between aggressive behaviour and injury in ice hockey. However, little is known about what can be done to reduce this behaviour to create a safer environment for the sport.
Existing reviews about reducing injury in sport have primarily assessed equipment or risk factors associated with injury.9–11 Recent systematic reviews highlighted the risks of bodychecking and renewed calls for policies to disallow bodychecking among youth playing ice hockey.3,12 We conducted a systematic review to assess the effectiveness of interventions designed to reduce aggressive acts and related injuries among ice hockey players. We were particularly interested in evaluating the effectiveness of rule changes, educational interventions and behavioural modification in reducing aggressive acts and related injuries.
Methods
Data sources
We searched 8 electronic databases for potentially relevant articles published from the time of the database’s inception through July 2012: MEDLINE (using the search engines Ovid [from 1950] and PubMed [from 1948]), Embase (from 1980), CINAHL (from 1981), Journals @ Scholars Portal (from 1960), the Cochrane Library (from 1980), PsycINFO (from 1987) and Web of Science (from 1976). For each search, we used a combination of Medical Subject Headings (MeSH) and key words, including “hockey,” “ice hockey,” “aggression,” “violence,” “anger,” “injury,” “wounds and injuries,” “injury prevention,” “prevention studies,” “intervention,” “intervention studies,” “prevention,” “reducing,” “protection” and “education.” (Details of the search strategy are provided in Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112017/-/DC1). Search terms were modified based on search results to generate increasingly inclusive sets of potentially relevant articles. We did not restrict these searches by language, publication year or publication status.
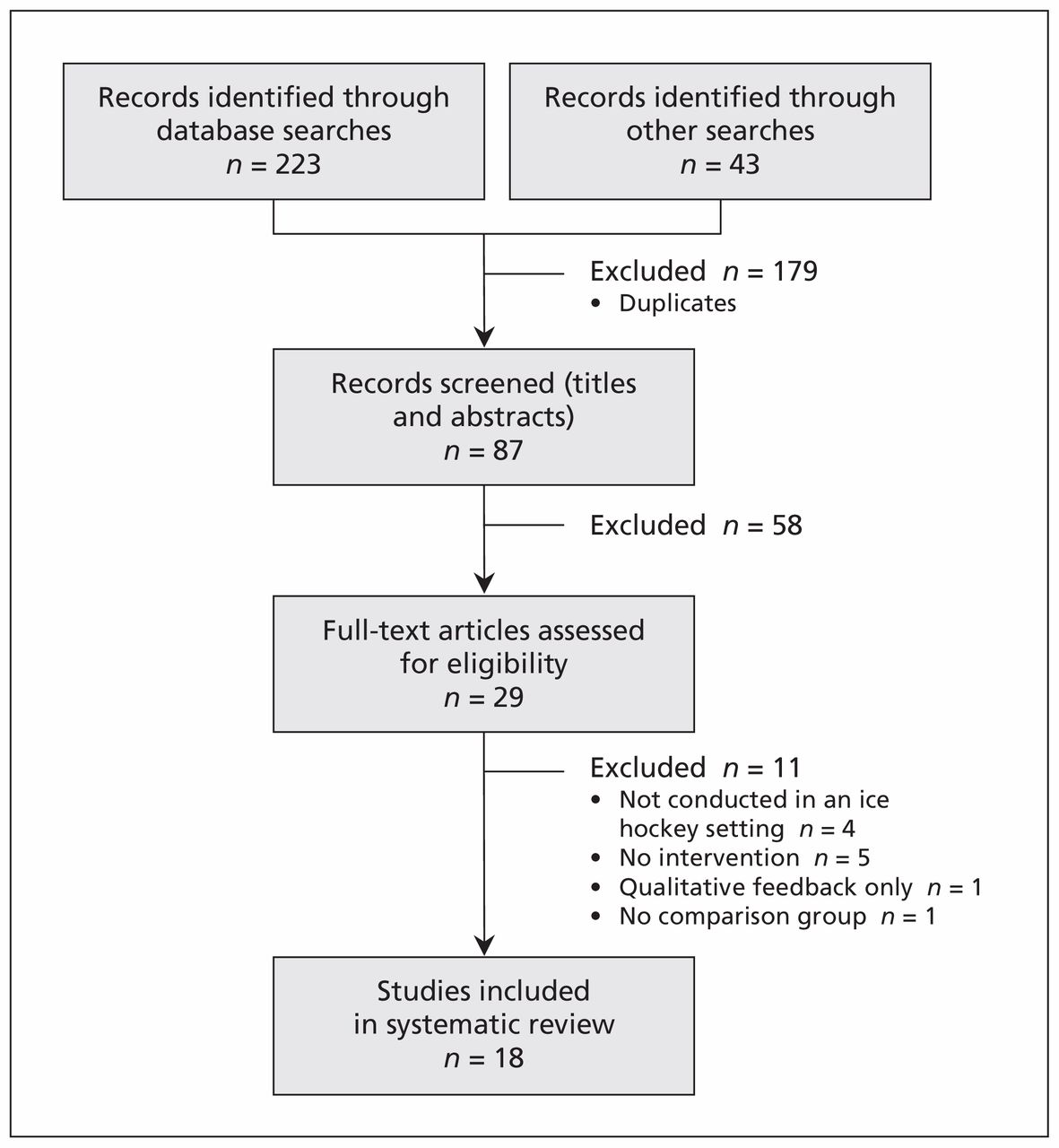
We also used the Internet search engines Yahoo!, Google, Google Scholar and Dogpile, with the same search terms as those listed above. We manually searched for related articles in 4 sports medicine journals (American Journal of Sports Medicine, British Journal of Sports Medicine, Injury Prevention, and Sports Medicine, all of which commonly publish articles related to ice hockey and injury prevention) from 2000 to 2010; all 5 volumes of Safety in Ice Hockey;13–17 and the bibliographies of all included studies. We reviewed the titles and abstracts of potentially relevant articles to identify studies that met our selection criteria (Figure 1).

Selection of articles for inclusion in the systematic review.
Study selection
We included studies of interventions applied directly to the hockey coaches or players that attempted to reduce aggressive behaviours in ice hockey, had a comparison group (cross-sectional, case–control, cohort, before–after, quasi-experimental and randomized controlled trial designs were all considered), and measured injuries, penalties or ratings of aggressive behaviour as outcomes. We excluded studies that applied to other types of hockey, involved only the use of protective equipment or were not conducted in an ice hockey setting.
Data extraction and synthesis
Two of us (S.N. and L.Z.) independently reviewed the articles of the included studies and extracted the data; the third author (M.D.C.) confirmed that the extraction of data was complete. We obtained data on the study design, the study population, the hypothesis or research question, the outcome measures, the study methods, the statistical analyses, the results and the conclusions. We assessed the methodologic quality of each study based on a checklist created by Downs and Black.18
The individual studies had considerable heterogeneity and varied by interventions, outcome measures and definitions of exposure. This heterogeneity precluded the ability to perform a meta-analysis.
Results
Included studies
Of the 29 full-text manuscripts retrieved for preliminary consideration, 18 were selected for inclusion in our review. We excluded 11 articles because the study did not assess aggression or injury related to players in an actual ice hockey setting (n = 4), there was no intervention (n = 5), only qualitative feedback from coaches was reported, or the study had no comparison group. (The citations of the excluded studies are provided in Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112017/-/DC1).
Of the 18 included studies, 13 assessed the effectiveness of changes in mandatory league rules,19–31 3 assessed the effectiveness of educational interventions,32–34 and 2 assessed the effectiveness of psychosocial interventions.35,36 Thirteen of the studies included youth players in minor leagues. One study involved players in Canada and the United States, 13 studies were completed solely in Canada, and 4 were completed in the United States. Characteristics of the included studies are summarized in Table 1.
Description of study characteristics
Quality assessment
Details of our assessment of the methodologic quality of the studies based on the criteria of Downs and Black18 are provided in Appendix 3 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112017/-/DC1). In brief, several studies19–22,24,26,28–31,34 drew on large samples, such as all hospital visits in multiple Canadian provinces. In some studies, confounding variables were difficult to control because of their retrospective or observational nature;25,26,30 and only one of the studies was randomized.33 No studies looked at broader outcomes such as the effects of injury on participation rates in hockey or advancement of players to higher or elite levels of play.
Effect of interventions
The effects of the interventions on aggressive acts and related injuries are summarized in Table 2.
Description of study outcomes, by type of intervention
Rule changes
Thirteen studies evaluated changes in mandatory rules intended to curb aggressive behaviour and subsequent injury.19–31 Three studies examined the Fair Play Program.20,21,23 This program includes sportsmanship as a component of the final standings, adapted from an experimental program created by Edmond Vaz.37 Points are awarded to teams at the end of every season or tournament for staying below a pre-established limit of team penalties per game.21 Nine studies investigated bodychecking rules.19,22,24,25,27–31 The remaining study examined legal punishment for aggressive illegal acts in professional hockey.26
The 3 studies of the Fair Play Program noted an overall decrease in the number or severity of penalties,20,21,23 and one also reported a decrease in injury rates.21
Most of the 9 studies evaluating the enforcement of rules prohibiting bodychecking observed reductions in penalties, injuries or both, and in many studies these differences were statistically significant. Seven of the 9 studies showed decreased injury rates.19,22,24,25,27,28,30 Typical of this group of studies, Regnier and colleagues19 noted more penalties in games in which bodychecking was allowed, along with a higher risk of serious injury among Peewee players (age 11–12 years). Macpherson and colleagues24 found that injury rates in boys’ minor hockey in Ontario and Quebec were higher in leagues in which bodychecking was allowed than in leagues in which it was not allowed. The players in leagues that allowed bodychecking were also more likely to experience a concussion or fracture. Among older players (age 14–15 years), all of whom were in leagues that allowed bodychecking, checking-related injuries were more common among those who had previous experience with it (Ontario leagues) than among those introduced to bodychecking for the first time (Quebec leagues); this difference suggests a protective effect of delaying the introduction of bodychecking. On the contrary, Kukaswadia and colleagues’ retrospective cohort study noted a beneficial effect of introducing bodychecking at an earlier age, but it excluded a large number of possible cases to control for confounding variables.29
One study examined the impact of legal punishment on the frequency of aggressive behaviour across the National Hockey League (NHL).26 After the Bertuzzi incident (a widely publicized incident of highly aggressive and injurious behaviour for which player Todd Bertuzzi received a high-profile legal charge), there was an insignificant reduction in the overall frequency of aggressive behaviour but a significant decrease in specific acts of aggression (fighting and game misconduct infractions).
Educational interventions
All 3 studies that evaluated the effectiveness of educational interventions showed a reduction in penalties, but they were not powered or designed to show a change in injury rates.32–34
In the only randomized controlled trial included in our review, Cook and colleagues33 evaluated the effectiveness of ThinkFirst Canada’s Smart Hockey video, which encourages respectful play to avoid injury and educates players and coaches about the diagnosis and treatment of concussion. This small study showed a decrease in the number of bodychecking-related penalties and the occurrence of aggressive and negligent behaviour, but it did not measure injury rates.
In a before–after study, Trudel and colleagues evaluated an intervention from the 1980s that introduced coaches to methods for properly teaching hockey skills through both video and training sessions.32 The authors reported a significant decrease in the number of penalties per game in only 1 of the 4 leagues that adopted the strategy and showed that the proportion of major injuries related to bodychecking dropped from 75.0% to 68.7% after the intervention.
Smith and colleagues performed a before–after study of the Hockey Education Program — the most multifaceted of the educational interventions designed to ensure youth players develop sportsmanship, skills and a Fair Play approach to the game.34 They found that the mean number of penalties per 100 games decreased in all 4 penalty sectors (tactical, minor, major and other) and that the percentage of Fair Play points increased throughout the 4 seasons studied.34
Psychosocial interventions
Two articles reported the effects of cognitive behavioural strategies used with individual hockey players to prevent their aggressive behaviour, but neither reported on the effects of such interventions on injuries.35,36 Mattesi reported an overall decrease in the percentage of penalty minutes after his aggression-management training was implemented among 3 players.35 In the study by Lauer and colleagues,36 the Playing Tough and Clean Hockey Program was found to help 2 of the 3 players enhance their ability to manage their emotions and decrease their aggressive behaviour.
Interpretation
In our review of the literature, we found that interventions based on rule changes showed the greatest likelihood of making ice hockey safer for youth. The introduction of the Fair Play Program in several Canadian and American ice hockey leagues has succeeded in reducing penalties; however, only 1 of the 3 studies of the program that we reviewed evaluated injury rates, and it showed a decline.21 Educational and psychosocial approaches were found to reduce aggression-related high-risk behaviours. Although existing studies of these approaches lacked the power to show reductions in injury rates, these interventions show promise.
Rule changes essentially alter the culture of a sport and clearly define acceptable behaviour for all stakeholders (players, coaches, parents and officials) simultaneously. Although educational interventions, such as the Smart Hockey video, can do this to a certain extent, their effectiveness depends on the involvement and simultaneous change in attitudes and behaviour of all stakeholders. For this involvement and change to occur, educational interventions need to be implemented consistently, associated with an intrinsic reward for the change and have widespread universal application. Such an effect occurred at the New Zealand Rugby Union: when rule changes were implemented along with mandatory nationwide educational programs for injury prevention at all levels, the number of neurologic injuries decreased significantly.38 More research is needed regarding mandatory rule changes combined with well-designed educational interventions implemented at a national level.
Introducing the Fair Play Program in conjunction with educational interventions and enforced rules holds promise in reducing injuries related to aggressive behaviour. Critics of the Fair Play Program’s practice of having a pre-established limit of team penalties per game argue that it may encourage teams to believe they are entitled to fill their penalty quotas and that it may limit the number of penalties referees call in high-stakes games.6 Removing quotas from the Fair Play Program and introducing stricter penalties for high-risk behaviours (e.g., hits to the head and bodychecking from behind), with a loss of points in the overall standings, may also improve the effectiveness of such systems.39 The Fair Play Program is already an accepted part of a minority of hockey organizations, so it could be a means by which to ultimately alter hockey culture.
A change toward different rules and their strict enforcement combined with universal education, structural changes in hockey governance, financial and other incentives for safe play and disincentives for unsafe play holds promise for curbing aggression-related injury.
Limitations
Most of the studies we reviewed were retrospective in nature. Although attempts were made in some studies to control for confounding factors, this is difficult to accomplish without randomization. The cardinal issues associated with selection bias, information bias and confounding with case–control and cohort studies need to be carefully considered. Randomization is a key to addressing these limitations in future studies of the effects of interventions that attempt to reduce aggression-related hockey injuries.
Variability in outcomes was another limitation. Some studies reported on penalty minutes, others measured injury reduction, and some reported on both. None of the studies assessed outcomes such as attrition from the sport or any positive aspects of aggression. The studies of educational and psychosocial interventions generally had smaller samples and were not designed to measure injury reduction.
Feasibility was not specifically addressed in any of the studies. However, studies that evaluated rule changes reported that the implementation of rule changes was achieved across large numbers of players. Cognitive behavioural approaches are time and resource intensive and likely of limited widespread acceptability. Experience from rugby has shown that educational approaches are in between these extremes but that universal nationwide implementation is possible.38 None of the studies assessed the cost-effectiveness of interventions — a characteristic closely associated with feasibility. Use of computer technology in future interventions, for example through the Web40 and smartphone applications, could make widespread implementation more cost-effective and feasible.
We were unable to identify any interventions based on economic incentives or disincentives, such as changes in fines, insurance premiums or salaries. A complete assessment of how to make ice hockey safer should include implementation and evaluation of such interventions.
All of the studies included in our review were from North America. Future research should also come from other countries.
Finally, we did not identify studies of legislative changes. However, research into bicycle safety has shown that such changes have the potential to alter behaviour and reduce injury rates.41
Conclusion
Several studies included in our review showed that changes to rules to limit the exposure of youth to bodychecking were associated with reduced rates of injury among ice hockey players. Other interventions, including the Fair Play Program, educational interventions and cognitive behavioural modification, had positive effects on reducing aggressive acts; however, more research is needed to determine whether these approaches reduce injury rates on their own. Well-designed multifaceted strategies that combine such approaches hold promise and should be the topic of future research.
Acknowledgements
The authors acknowledge Dr. David Lightfoot for his assistance in searching the literature, and Sharon Nancekivell and Shudong Zhang for their editorial assistance in preparing the manuscript for submission.
Michael Cusimano leads the Canadian Brain Injury and Violence Research Team.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Michael Cusimano conceived of the study, and Sofia Nastis and Laura Zuccaro performed the literature search. All of the authors performed the critical appraisal and analysis of findings, wrote and revised the manuscript and approved the final version submitted for publication.
Funding: This study was funded by a Canadian Institutes of Health Research Strategic Team Grant in Applied Injury Research in partnership with the Ontario Neurotrauma Foundation (grant no. TIR-103946). The opinions are those of the authors and not of the funding agencies.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Association of in-competition injury risk and the degree of rapid weight cutting prior to competition in division I collegiate wrestlers
- Understanding the resistance to creating safer ice hockey: essential points for injury prevention
- Can legislation aimed at preventing sports-related concussions in youth succeed?
- Effectiveness of an educational video on concussion knowledge in minor league hockey players: a cluster randomised controlled trial
More in this TOC Section
Similar Articles

