


- © 2007 Canadian Medical Association
A 71-year-old woman presented to the emergency department with a 6-week history of recurrent diffuse abdominal pain and nausea without vomiting that was unrelated to food consumption and was unaccompanied by fever or weight loss. The patient had a history of type 2 diabetes mellitus that had been treated with metformin (850 mg/d). Outpatient investigations, including gastroscopy, abdominal ultrasonography, gynecological examination and colonoscopy performed 5 days before presentation, yielded normal results. The patient was admitted to hospital with acute renal failure.
The results of a physical examination on admission were within normal limits. An electrocardiogram and a chest radiograph appeared normal, as were the patient's vital signs. Test results showed elevated levels of blood urea nitrogen (14.3 [normal 2.9–8.9] mmol/L), serum creatinine (265 [normal 44–150] μmol/L) and phosphorus (1.58 [normal 0.81–1.45] mmol/L) and a decreased calcium level (2.07 [normal 2.15–2.58] mmol/L). The results of urine analyses showed a sodium level of 65 (normal 100–260) mmol/L) and 130 mg protein per 24 hours. In addition, a few erythrocytes and leukocytes and no casts were observed in the urine. The estimated glomerular filtration rate (achieved by use of an abbreviated Modification of Diet in Renal Disease [MDRD] Study equation) was 16 (normal > 90) mL/min per 1.73 m2. The test results for liver function were normal and for hepatitis antibodies were negative. Glycosylated hemoglobin was 6.4% (normal < 6%) and the hemoglobin level was 115 (normal 121–151) g/L. The results of an abdominal CT scan, a gastrointestinal barium series, endoscopic ultrasonography and a renogram were normal. The patient's medical records showed that 2 months before presentation her serum creatinine level had been normal (106 μmol/L) and that there was no microalbuminuria.
The patient continued to have occasional abdominal pains, and a painful symmetric sensory polyneuropathy (“glove and stocking” type) developed. The erythrocyte sedimentation rate was 43 (normal 0–20) mm/h and the C-reactive protein level was 21 (normal < 6) mg/L. The immunofluoresence for antinuclear antibodies was graded as +1. The results of protein immunoelectrophoresis, rheumatoid factor, antiphospholipid and antineutrophil cytoplasmic antibodies were negative, and the serum complement was normal.
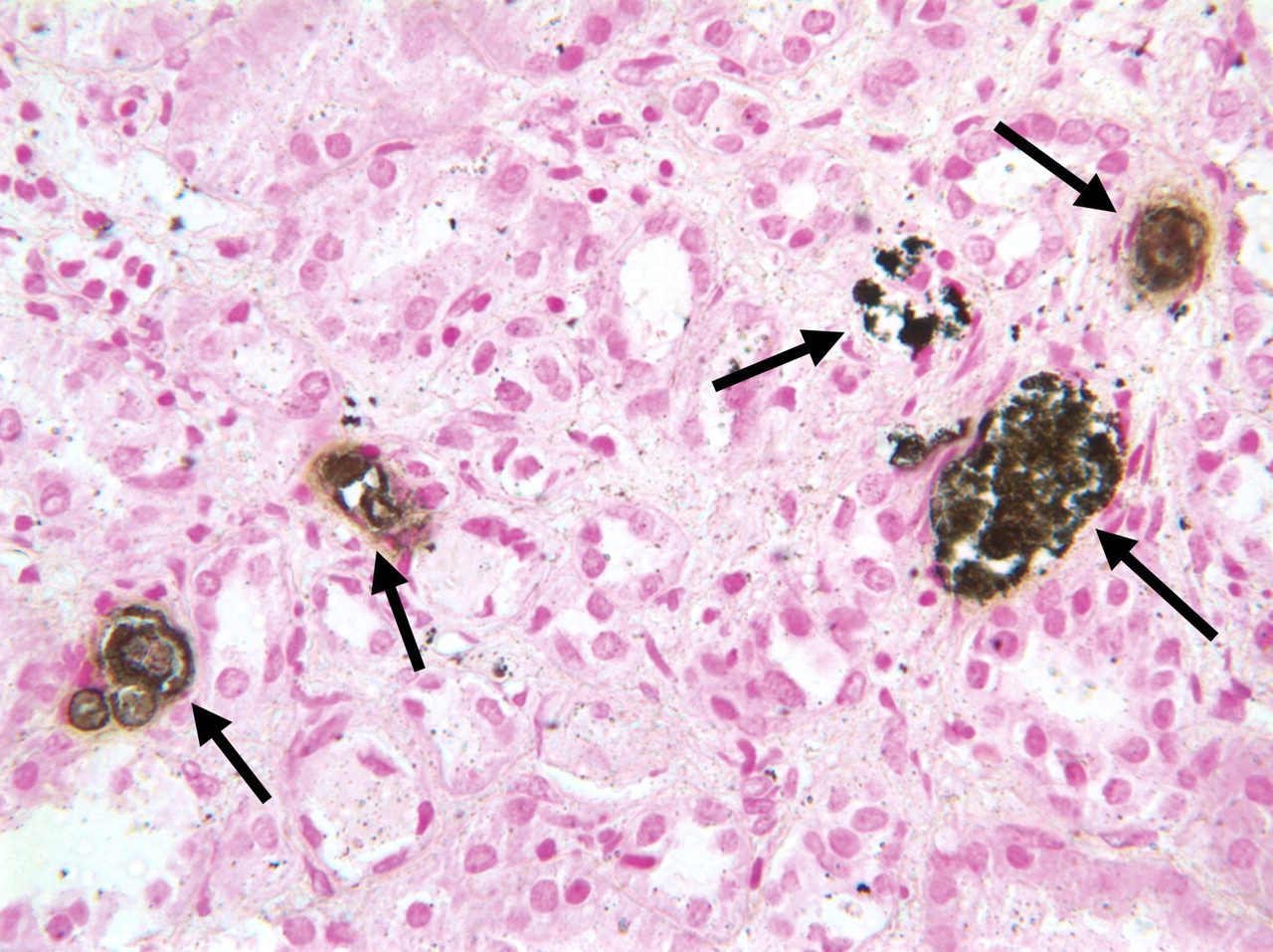
A kidney biopsy showed 7 normal glomeruli with mild thickening of Bowman's capsule. However, the main finding was atrophy of the tubuli with thinning of the epithelium, widespread interstitial fibrosis, focal mononuclear infiltrates and prominent, extensive calcium deposits (Figure 1) in the tubular lumina (i.e., nephrocalcinosis). The results of immunofluorescence for the detection of immunoglobulins and complement were negative. The results of histologic investigations were highly suggestive of phosphate nephropathy; thus, we investigated the bowel preparation that had been used before the patient's colonoscopy, performed 5 days before presentation to the emergency department. We found that the patient had received a preparation of disodium hydrogen phosphate and sodium hydrogen phosphate, which contained 370.8 mmol (6.6 g) sodium hydrogen phosphate.

Figure 1: A kidney biopsy showing tubular atrophy and multiple calcium deposits (arrows) within the tubules (hematoxylin–eosin stain, original magnification × 400).
Although an explanation for the patient's abdominal pain and peripheral neuropathy was not immediately apparent, we hypothesized that her symptoms may have been related to an evolving rheumatic condition. The patient's abdominal pains spontaneously resolved after 2 months. However, the glomerular filtration rate did not improve.
Acute hyperphosphatemia associated with oral phosphate used for bowel cleansing has long been recognized.1 However, renal failure caused by oral phosphate preparations has only recently been established as a distinct entity.2–4 Ingestion of oral sodium phosphate as a bowel purgative before colon-imaging studies may be followed by an acute increase in serum phosphate that can lead to calcium phosphate deposits in the kidney tubules and subsequent tubulointerstitial nephropathy. The frequency of colon examinations is increasing and oral phosphate purgatives are more acceptable to patients than other regimens;5 thus, this condition may not be uncommon. In a recent study, 21 of 31 native renal biopsies with nephrocalcinosis were from patients who were normocalcemic and had had a recent colonoscopy involving an oral phosphate solution for bowel preparation.4 After a mean follow-up of 16.7 months, 4 of the 21 patients were receiving long-term hemodialysis and 17 had developed chronic irreversible renal failure, as did our patient.
Several factors may predispose a patient to acute phosphate nephropathy. These include female sex, greater than 60 years of age, earlier subclinical renal dysfunction (e.g., caused by hypertension or diabetes) and the use of angiotensin-converting-enzyme inhibitors or angiotensin-receptor blockers.3,4 For older patients (i.e., > 60 years of age) who present with unexplained acute renal failure, physicians should inquire whether the patient has had a recent colonoscopy and what method of bowel preparation was used.4 Patients who are at risk of acute hyperphosphatemia should receive alternative preparations before colonic procedures.
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

