


- © 2007 Canadian Medical Association
The case: A 37-year-old man was admitted to our hospital with recurrent palpitations. Arrhythmogenic right ventricular cardiomyopathy had been diagnosed 10 years before admission and had been treated with sotalol. Physical examination revealed a blood pressure of 160/98 mm Hg and a heart rate of 150 beats/min, but no other abnormalities. An electrocardiogram showed ventricular tachycardia (Fig. 1) that, after an intravenous infusion of procain-amide, converted to sinus rhythm with epsilon waves and T-wave inversions in the precordial leads (Fig. 2). An echocardiogram showed that the right side of the heart was dilated in the absence of intracardiac shunts and that there was impaired left ventricular function with regional wall-motion abnormalities. Cardiac catheterization, performed to exclude coronary artery disease, showed normal coronary arteries. The patient was referred for cardiac magnetic resonance imaging.

Fig. 1: Electrocardiogram obtained on admission showing monomorphic ventricular tachycardia with left superior axis and left bundle branch block–type configuration, indicating origin in the right ventricle.

Fig. 2: Electrocardiogram showing typical epsilon waves in precordial lead V1 (inlay, arrow) and inverted T waves in precordial leads V1 through V3.
Spin echo images showed a thinned right ventricular free wall and focal hyperintensity suggestive of fatty infiltration at the level of the apex and right ventricular free wall (Fig. 3). Typical focal dyskinetic bulging in the free wall of the right ventricle was seen on cine imaging (Fig. 4, D and E). The left ventricle also showed regional wall thinning with wall-motion abnormalities in the inferoposterolateral region and moderate impairment of global left ventricular function (Fig. 4, A and B). Late gadolinium-enhanced images showed various areas of hyperenhancement in the inferoposterolateral region, septum and right ventricular free wall (Fig. 4, C and F). See videos online at www.cmaj.ca/cgi/content/full/176/13/1819/DC1.

Fig. 3: Transaxial spin echo image showing thinned right ventricular free wall, with high signal intensity in the apex and free wall suggestive of fatty infiltration (arrowheads). Note: RV = right ventricle, LV = left ventricle.

Fig. 4: Upper panel: Three-chamber cine image in the diastolic (A) and systolic (B) phases, and a late gadolinium-enhanced image (C). Marked thinning of the posterolateral left ventricular wall with dyskinesia (A and B, arrow) and focal regions of fibrosis (C, open arrowheads) in the left ventricle are shown. Lower panel: Mid-ventricular short-axis cine image in the diastolic (D) and systolic (E) phases, and a late gadolinium-enhanced image (F). Dyskinetic bulging of the right ventricular free wall (E, arrowhead) is visible, with corresponding fibrofatty replacement (F, asterisks). Areas of fibrous tissue in the left ventricle (F, arrowheads) correspond with the regions of fibrosis on the 3-chamber view (C).
The combination of ventricular tachycardia of right ventricular origin, epsilon waves on the electrocardiogram, right ventricular aneurysms and the findings of cardiovascular magnetic resonance imaging in the left ventricle in the absence of coronary artery disease were diagnostic of arrhythmogenic right ventricular cardiomyopathy with biventricular involvement. The patient had symptoms of ventricular arrhythmia despite adequate sotalol therapy; thus, catheter ablation was considered but was unsuccessful because of multiple foci. Despite a lack of evidence in the literature, the patient was given amiodarone therapy. He showed a favourable response and was still free of symptoms on follow-up 3 years later.
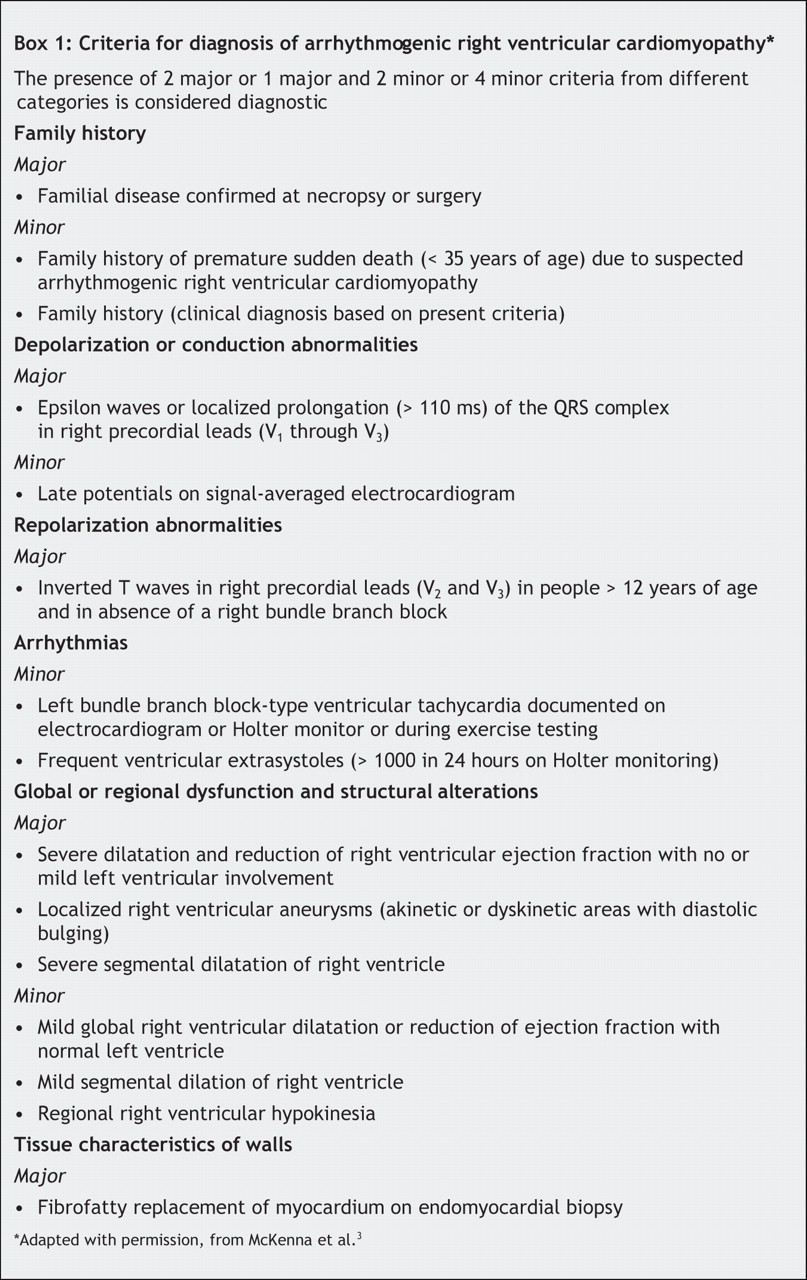
Arrhythmogenic right ventricular cardiomyopathy is a disease of the right ventricle of the heart with a genetic basis. It is characterized by myocardial atrophy and fibrofatty replacement, and ventricular arrhythmias.1–3 The disease is commonly inherited as an autosomal dominant trait with incomplete penetrance, although recessive forms have been described.4 The prevalence in the general population is about 1 in 5000, and it is an important cause of sudden cardiac death in young adults.5,6 This pathological diagnosis is difficult to establish in clinical practice; thus, an expert consensus group has proposed criteria to allow confirmation of the diagnosis (Box 1).3 Genetic analysis, although in its infancy for this disease, may be incorporated into the diagnosis of familial arrhythmogenic right ventricular cardiomyopathy among first-degree relatives with incomplete disease expression.4
Long-term studies have shown arrhythmogenic right ventricular cardiomyopathy to be a progressive disease that may not be confined to the right ventricle. The left ventricle is involved in about 76% of cases (demonstrated by histopathology). Left ventricular involvement is associated with clinical arrhythmic events and, compared with cases of isolated right ventricular involvement, is associated with more severe cardiomegaly, inflammatory infiltrates and heart failure.1,6
Arrhythmogenic right ventricular cardiomyopathy has anatomic, functional and tissue-specific characteristics; thus, cardiovascular magnetic resonance imaging is an ideal technique for diagnosis.4 It allows evaluation of regional wall-motion abnormalities, increased right ventricular volumes, local aneurysms, increased signal intensity suggestive of fatty infiltration and hyperenhancement of fibrous areas after injection of a contrast agent. Cardiovascular magnetic resonance imaging is a valuable technique in the diagnostic work-up of arrhythmogenic right ventricular cardiomyopathy, but should be part of a full noninvasive evaluation that includes a 12-lead electrocardiogram, a signal-averaged electrocardiogram, an exercise test and ambulatory electrocardiogram monitoring.
Treatment of arrhythmogenic right ventricular cardiomyopathy involves pharmacologic suppression of malignant arrhythmias in symptomatic patients, or catheter ablation which is often unsuccessful because of the progressive nature of this disease.5 Automatic implantable defibrillators are still considered the most effective treatment to prevent sudden cardiac death.
Footnotes
-
See videos online showing regional wall thinning of the left ventricle and dyskinetic bulging of the right ventricle (available at: www.cmaj.ca/cgi/content/full/176/13/1819/DC1).
This article has been peer reviewed.
Competing interests: None declared.
In this issue
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

