


A 15-year-old girl presented with a sudden onset of abdominal and chest pain, nausea and postprandial gastric fullness. She had a history of an eating disorder with low weight and amenorrhea of 6 months' duration. On physical examination, her weight, height and body mass index were 160.5 cm, 37.0 kg and 14.4 (normal 18.5–25.0) kg/m2 respectively. She had subcutaneous emphysema in her neck and epigastric tenderness on examination. Laboratory investigations showed a low free triiodothyronine level (3.15 [normal 3.63–7.68] × 10–3 nmol/L]) and ketonuria.
A barium study of the upper gastrointestinal tract showed significant dilatation of her stomach and of the second and third portions of her duodenum as well as duodenal obstruction (Fig. 1), which was consistent with superior mesenteric artery (SMA) syndrome. Fortunately, no perforations of the esophagus, stomach or duodenum were detected. A CT scan of the cervical spine, chest and abdomen showed subcutaneous emphysema, pneumomediastinum, spinal epidural emphysema, retroperitoneal emphysema and a remarkably dilated stomach (Fig. 1). About 3 000 mL of gastric fluid was aspirated through a nasogastric tube, with resolution of the gastric fullness and discomfort.
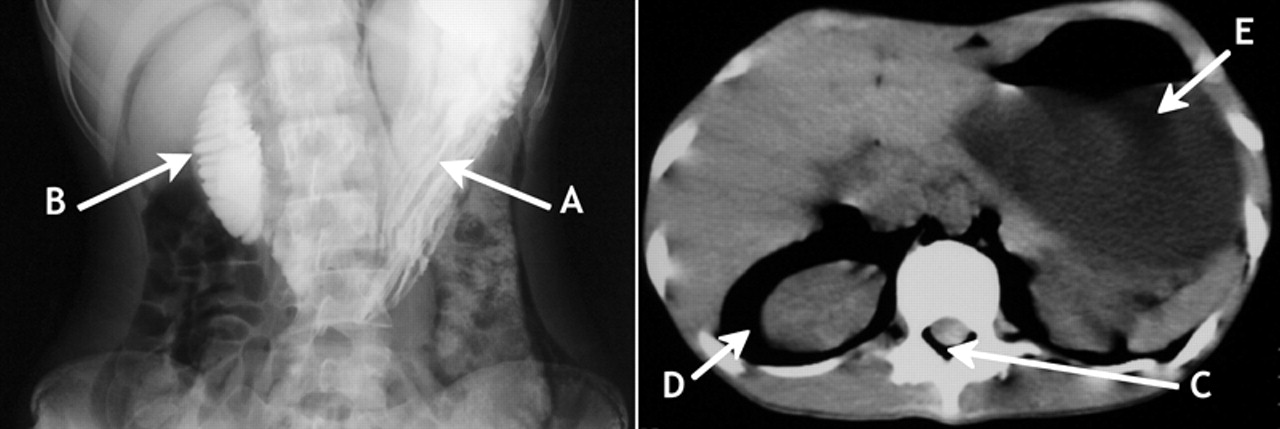
Fig 1: Left: Barium study, showing dilatation of the stomach (A) and the second and third portions of the duodenum, and obstruction of the duodenum (B). Right: CT scan of cervical spine, chest and abdomen, showing subcutaneous emphysema, pneumomediastinum, spinal epidural emphysema (C), retroperitoneal emphysema (D) and dilated stomach (E).
The patient agreed to parenteral hyperalimentation for 2 weeks. Her symptoms improved, and a CT scan showed resolution of the gastric dilatation and subcutaneous emphysema.
SMA syndrome is a rare cause of small-bowel obstruction. It is thought to be the result of compression of the third portion of duodenum between the aorta and vertebral column posteriorly and the superior mesenteric neurovascular bundle anteriorly. SMA syndrome is caused by eating disorders in 30% of cases,1 probably because of the loss of the cushion of fat that surrounds the neurovasucular pedicle,2 but the syndrome may also result from a complication of scoliosis surgery. Presenting symptoms include postprandial epigastric pain, eructation, fullness and vomiting. Weight gain appears to be important for the treatment of SMA syndrome.
Why subcutaneous emphysema developed in our patient is unclear, since it usually occurs secondary to surgical, dental and endoscopic procedures, or spontaneously in people with asthma. Our patient may have had fragile connective tissue in the pleural cavity owing to malnutrition,3 and increased intra-abdominal or intrapleural pressure owing to the SMA syndrome, which, in addition to the vomiting caused by the gastric obstruction, forced air into the subcutaneous tissues.
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

