

A 78-year-old man presented with bilateral leg edema, pleural effusions and elevated cholestatic liver enzyme levels that had worsened over two years. Magnetic resonance cholangiopancreatography scans suggested sclerosing cholangitis (Figure 1A). Positron-emission tomography–computed tomography scans showed bilateral pleural effusions with right-side predominance, thickening of the pleuropericardial wall and accumulation of fluorodeoxyglucose in the right pleura (Figure 1B). Cardiac catheterization showed bilateral elevation of ventricular end-diastolic pressure with a square root sign (Figure 1C), which suggested constrictive pericarditis. Pleuroscopy identified milky white pleural plaques (Figure 1D). Because all three lesions shared the characteristic of slowly progressive fibroinflammation, immunoglobulin G4 (IgG4)-related disease was suspected. The patient’s serum IgG4 level was elevated at 7.60 (normal 0.01–1.40) g/L. Pleural biopsy specimens showed lymphoplasmacytic infiltration associated with hyalinized fibrosis (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160186/-/DC1). Immunostaining showed a cell count of 100 IgG4-positive plasma cells per high-power field, with an IgG4:IgG ratio of 70% (Appendix 1). One month after administration of prednisolone, no pleural effusions were seen on chest radiograph and liver enzyme levels were normal. The constrictive pericarditis persisted, requiring pericardiectomy to achieve clinical improvement. Pericardial biopsy specimens were consistent with IgG4-related disease (Appendix 1). We conclusively diagnosed IgG4-related pleuritis, sclerosing cholangitis and constrictive pericarditis. The case met the diagnostic criteria for IgG4-related disease.1
{kind=link}
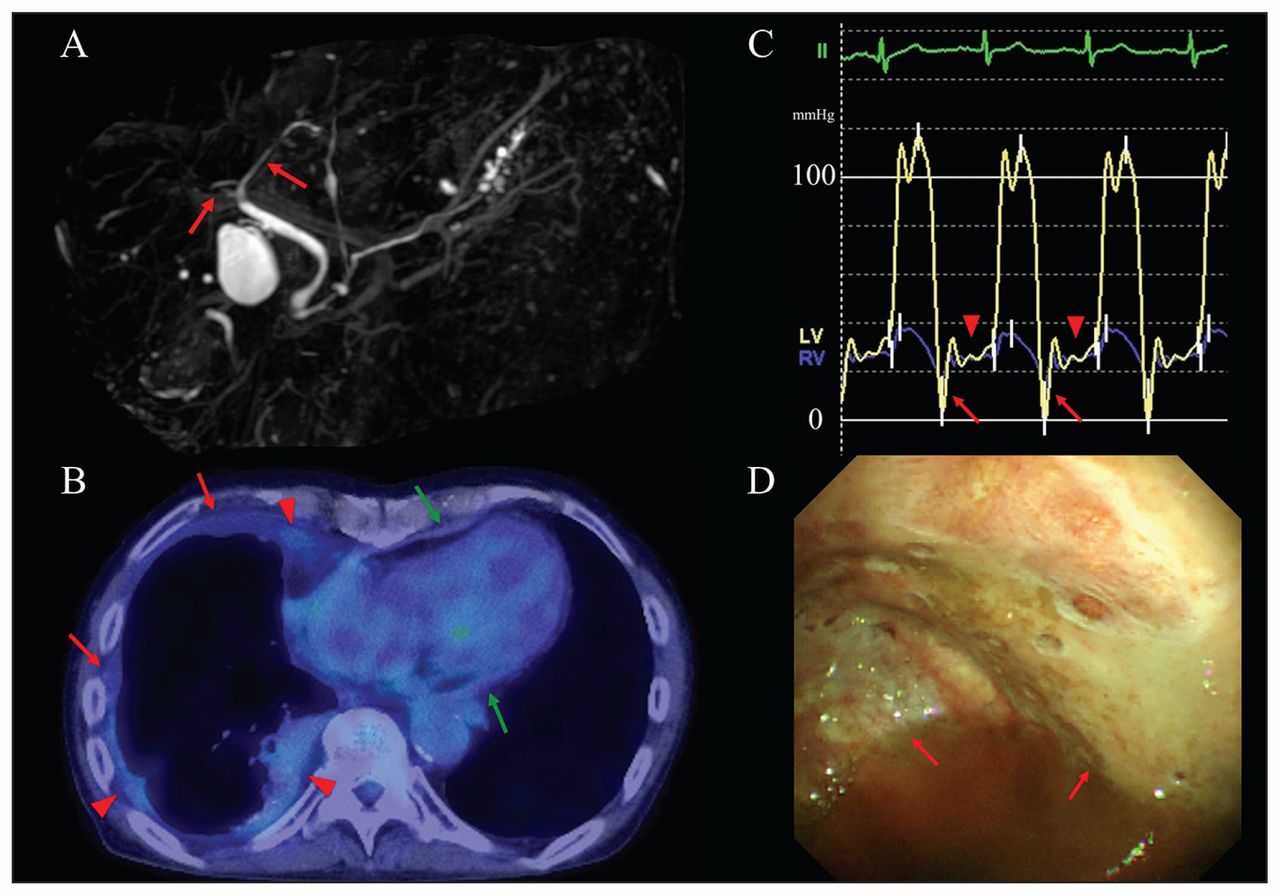
(A) Magnetic resonance cholangiopancreatography showing a long stricture of the intrahepatic bile ducts without prestenotic dilatation (arrows). (B) Positron-emission tomography–computed tomography scan showing bilateral pleural effusions with right-side predominance; thickening of the pleura on the right side (red arrows) and of the pericardial wall (green arrows) without calcification; and accumulation of fluorodeoxyglucose in the pleura on the right side (arrowheads). (C) Cardiac catheterization showing increased right ventricular end-diastolic pressure, a square root sign in the right and left ventricular diastolic pressure tracings (dip [arrows] and plateau [arrowheads]), and equalization of the right and left ventricular diastolic plateau pressure tracings (arrowheads). (D) Right-side pleuroscopy showing milky white pleural plaques suggestive of hyalinized collagen fibre deposits (arrows).
Immunoglobulin G4–related disease is a systemic fibroinflammatory condition characterized by simultaneous or heterochronic excessive lymphoplasmacytic infiltration of IgG4-positive plasma cells into various organs. It is analogous to systemic diseases such as systemic collagen vascular disease, lymphoproliferative disorders and tuberculosis. It occurs mostly in men, the average age of patients is about 60 years, and clinical manifestations are diverse depending on the affected organ.2,3 Patients often present with sclerosing cholangitis and rarely with pleuritis and pericarditis.2
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.