


A 72-year-old man developed a bluish, painless and rapidly enlarging lesion on the palm side of his ring finger, over the course of a few weeks. It was solid and 20 mm in diameter on examination (Figure 1A). A plain radiograph of the lesion showed well-circumscribed, subcutaneous multilocular calcium deposits without bony involvement (Figure 1B). The patient’s serum calcium and phosphate levels were normal.
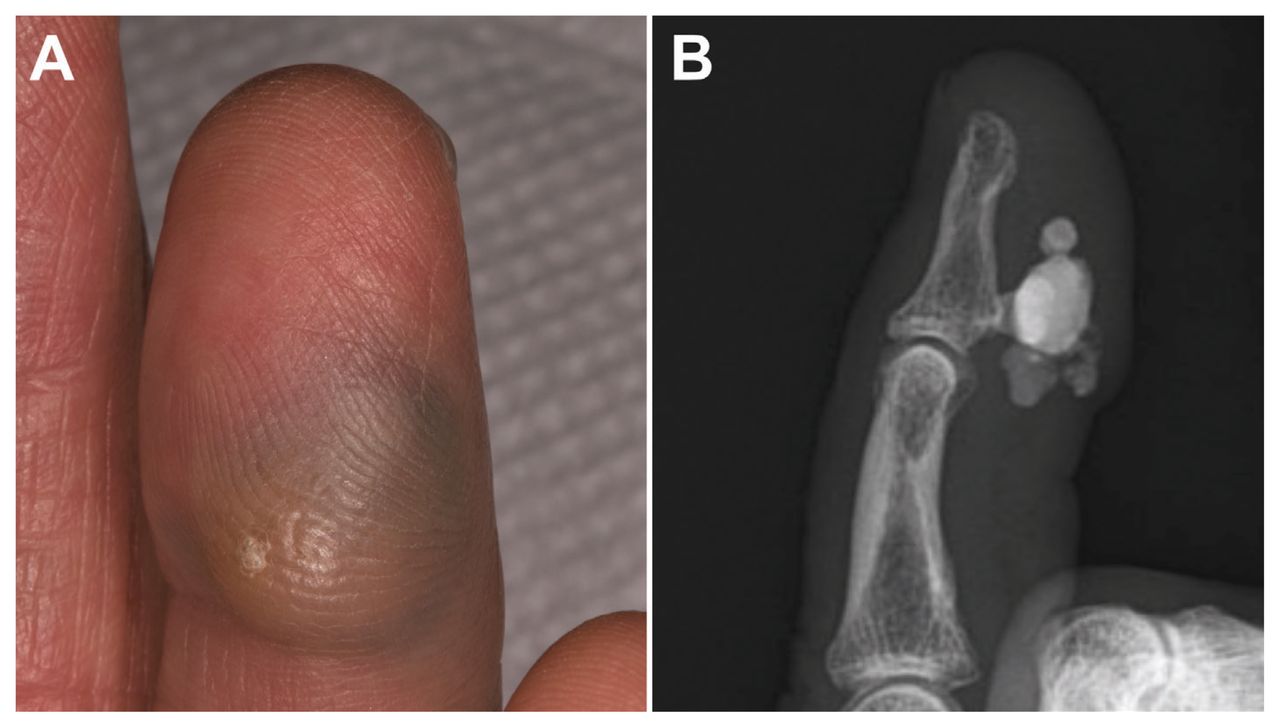
Clinical and radiographic images of pencil-core granuloma in a 72-year-old man. (A) We observed a bluish lesion of 20 mm in diameter on the palmar side of the ring finger. (B) Finger radiograph of the affected digit shows well-circumscribed, multilocular calcium deposits with no bony destruction.
Although we considered melanoma in the differential diagnosis, pencil-core granuloma was more likely because the patient had a history of a childhood pencil stab injury on the same finger. We excised the lesion and gross pathology revealed multiple blue-black nodules. Histopathology showed degenerative tissue with marked calcification and foreign body reaction, with histiocytes containing fragmented, coarse black particles. We diagnosed pencil-core granuloma.
Pencil-core granuloma is characterized by a delayed granulomatous foreign body reaction against degraded and diffusely dispersed graphite, the main component of pencil-core materials.1 Because pencil lead is a ceramic composite of graphite and clay and is sealed with waxes, it does not elicit immediate reactions. However, the core can gradually decompose over decades, dissolve and be phagocytosed, resulting in a granulomatous reaction.1
Melanoma, blue nevus and hemangioma should be in the differential diagnoses, owing to their similar clinical presentations.2 However, they rarely present with the calcinosis that can be seen in pencil-core granuloma, in which dystrophic calcification develops in degenerated or necrotic tissue derived from phosphate-bound denatured proteins and promoted by degenerated collagen tissue.3 Surgical removal effectively treats pencil-core granuloma. Immunohistochemical studies with HMB-45 and Melan-A can aid diagnosis as they are specific antibodies for melanoma detection.
This image highlights the importance of identifying multilocular calcium deposits by plain radiography to help clinicians differentiate benign pencil-core granuloma from malignant melanoma in patients with growing, blue-black, solid nodules.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

