

- © 2008 Canadian Medical Association
A 75-year-old woman with stage IV lung adenocarcinoma was admitted to our hospital to receive chemotherapy and a transfusion because of anemia. One unit of packed red blood cells was transfused via a pressure infusor into a Port-a-Cath, which had been implanted in the left side of her chest wall 2 years before. Within 1 hour of the start of the transfusion, the patient complained of dyspnea and retrosternal dull chest pain with a feeling of heaviness. The transfusion was stopped immediately. On physical examination, she appeared pale and weak. Her blood pressure was normal (130/60 mm Hg), but she had tachypnea (respiratory rate 24/minute) and tachycardia (pulse 130 beats/min). The pulse oximetry saturation was 90% at room air pressure. Auscultation of her heart and lungs was unremarkable except for crackles heard in the area of known neoplastic inflitrate. We compared a new chest radiograph with one that had been taken 3 weeks earlier and found a new widening of the mediastinum (Figure 1). Her cardiac enzyme levels were normal, but her hemoglobin level had declined from 89 g/L to 63 g/L. An electrocardiogram (ECG) showed atrial fibrillation with rapid ventricular response. No important ST-segment or T-wave changes or right heart strain pattern was noted. The patient had no history of hypertension or other cardiovascular diseases.

Figure 1: Left: A radiograph of the chest of a 75-year-old woman with stage IV lung adenocarcinoma taken 3 weeks before a red blood cell transfusion. The tip of a Port-a-Cath is indicated by the arrow. Opacities in the upper left and lower right lung can also be seen. Right: A chest radiograph showing mediastinal widening. This radiograph was obtained 1 hour after the transfusion was stopped because of dyspnea and retrosternal dull chest pain with a feeling of heaviness.
-
Aortic dissection
-
Transfusion-related acute lung injury
-
Mediastinal hematoma
-
Pulmonary embolism
-
Acute coronary syndrome
What is your diagnosis?
-
Arrange an urgent computed tomography (CT) scan of the chest
-
Initiate empiric anticoagulation with heparin
-
Administer intravenous steroids
-
Obtain a percutaneous biopsy of the mediastinum
-
Watchful waiting
What is your next step?
Discussion
The answer is (c): a mediastinal hematoma due to a Port-a-Cath complication and the next best step is (a): arrange an urgent CT scan of the chest. This diagnosis was supported by several nonspecific findings (including the timing of the patient's symptoms, her normal blood pressure, widened mediastinum with a particular pain quality and her decreased hemoglobin level) and was confirmed by a CT scan of her chest (Figure 2). The tip of the Port-a-Cath, which had likely abutted the wall of the left brachicephalic vein for some time (Figure 3), created local erosion. This erosion ruptured the vein wall leading to a mediastinal hematoma when pressure was applied by the pressure infusor.
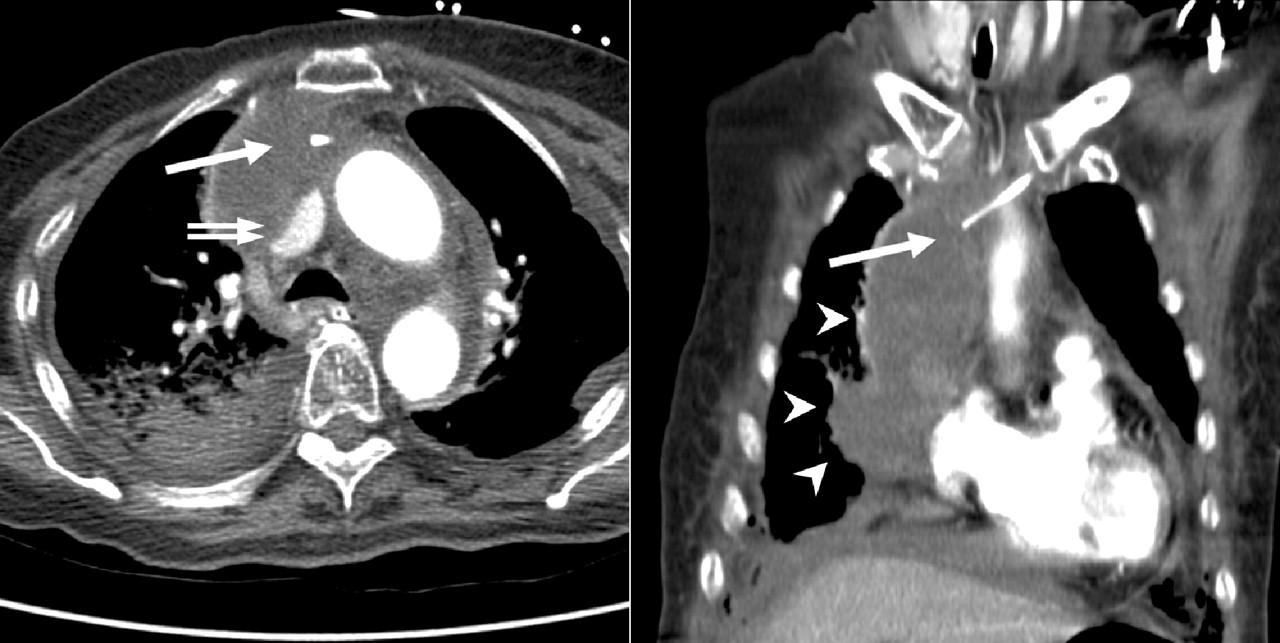
Figure 2: Contrast-enhanced CT scan of the chest revealed a right mediastinal hematoma (arrow heads) compressing the superior vena cava (double arrow) and extrusion of catheter tip (arrow).

{kind=link}
{kind=link}
{kind=link}
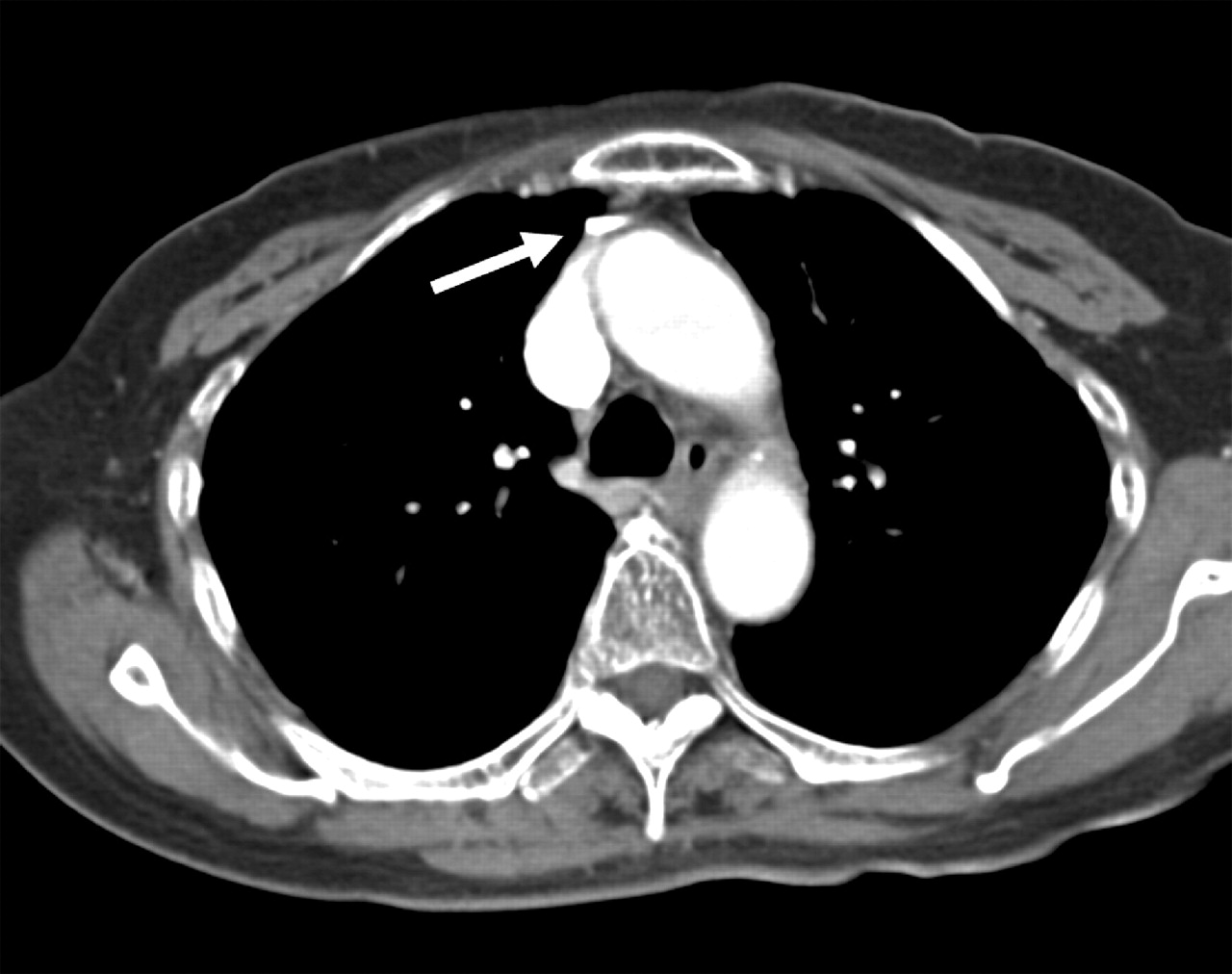
Figure 3: Contrast-enhanced CT taken 2 months before the red blood cell transfusion. On retrosepctive review, it was noted that the catheter tip (arrow) was abutting the vessel wall with anterior tension.
A mediastinal hematoma is often caused by blunt chest trauma and rupture of aortic aneurysms. It is also a rare complication of central venous catheter insertion and tends to occur within 1 week of catheter insertion.1,2 Patients often present with sudden onset dyspnea or chest pain, and chest radiographs often show mediastinal widening and unilateral or bilateral pleural effusions.2 Abutment of the catheter tip against a vein wall is often overlooked on chest radiographs used to confirm the catheter placement. An appropriate position of the catheter tip is parallel to the superior vena cava. A retrospective review of our patient's radiograph taken 3 weeks before presentation (Figure 1) shows that the catheter tip is not in the correct location.
Differential diagnosis: Although suggestive of aortic dissection, acute development of a widened mediastinum is not specific to aortic dissection. Patients with aortic dissection classically report a sudden, intense tearing or knife-like pain; however, our patient did not report these symptoms. In addition, about 70% of patients with aortic dissection have pre-existing hypertension,3 which was also not the case for our patient. Other common but nonspecific signs of aortic dissection, such as decreased peripheral pulse and a murmur of aortic regurgitation, were absent in our patient.
Transfusion-related acute lung injury commonly manifests as dyspnea, cough, fever, hypotension and sometimes frothy sputum. These symptoms typically begin within a few hours of starting a transfusion.4,5 The timing of our patient's symptoms were consistent with acute transfusion-related lung injury; however, the chest radiograph, which showed an absence of alveolar and interstitial infiltration and involvement of both lung fields, did not support this diagnosis.
Without ECG or myocardial enzyme evidence of an acute coronary syndrome, this diagnosis was effectively ruled out. Although we couldn't rule out a pulmonary embolus, based on our patient's initial presentation, a plausible alternative diagnosis explaining the mediastinal widening made this diagnosis less likely. The CT scan of our patient's chest, which better characterized the mediastinum, also ruled out this cause.
Footnotes
-
CMAJ invites submissions to “What is your call?” Clinical details (including images) are presented on the first page along with a multiple-choice question about the diagnosis. The answer and a brief discussion of the condition follow on the second page. We specifically invite submissions illustrating common or important radiographic and electrocardiographic diagnoses of appeal to a general audience. We allow up to 5 references and require authors to obtain consent from the patient for publication of his or her story (form available at www.cmaj.ca/authors/checklist.shtml).
Competing interests: None declared.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.