

Ever since the introduction of the concept of gestational diabetes mellitus, there has been controversy about the importance of this condition and the appropriateness of screening for it. Societies and associations such as the American College of Obstetricians and Gynecologists,1 the American Diabetes Association (ADA),2 the Canadian Diabetes Association3 and the Fourth International Workshop-Conference on Gestational Diabetes Mellitus4 have recommended either universal or selective screening. These recommendations are based on the premise that identification and treatment of gestational diabetes will avert some of the adverse outcomes that have been associated with this condition, such as pregnancy- induced hypertension, macrosomia (potentially associated with fetal birth trauma), perinatal mortality and neonatal metabolic disorders.5,6,7,8,9 Other bodies, such as the Canadian Task Force on the Periodic Health Examination10 and the Society of Obstetricians and Gynaecologists of Canada,11 have taken a more cautious approach, noting that there is insufficient scientific data to suggest that identification and treatment of gestational diabetes result in better maternal and neonatal outcomes. Indeed, there is evidence that identification of gestational diabetes may result in unfavourable maternal outcomes.12 Hunter and Keirse,13 in their contribution to Effective Care in Pregnancy and Childbirth, concluded that “except for research purposes all forms of glucose tolerance testing should be stopped.” Thus, it is important that studies be conducted to determine whether identification and treatment of gestational diabetes is associated with improvement in maternal and neonatal outcomes.
In this issue of CMAJ (page 403), Christian Ouzilleau and colleagues14 report their retrospective study of 300 pregnant women who had abnormal results on screening with a randomly administered 50-g glucose load and who subsequently underwent a follow-up 3-hour, 75-g oral glucose tolerance test (OGTT). These women received minimal or no therapeutic interventions. They were compared with a group of 300 pregnant women whose results on the initial screening were normal. The incidence of macrosomia was similar in the 2 groups.
The authors went on to look at the correlation between birth weight and 3 separate sets of plasma glucose values: on screening (1 hour after a 50-g glucose load), while fasting and 2 hours after a 75-g load. In each of these 3 analyses, progressively increasing plasma glucose values were associated with a progressive increase in birth weight, although the correlation was weak in each case.
The authors also performed multiple regression analysis to see if plasma glucose values while fasting and 2 hours after the 75-g glucose load remained independent predictors of birth weight. In both cases, plasma glucose remained an independent predictor, but the correlation was even weaker than in the initial analyses. The multiple regression analysis also showed that prepregnancy weight, weight gain during pregnancy and parity had a significant positive association with birth weight. Conversely, smoking had a significant but negative correlation with birth weight. Smoking, prepregnancy weight, weight gain during pregnancy and parity had higher correlations with birth weight than either fasting plasma glucose or plasma glucose 2 hours after a 75-g load. These results confirm the work of others, demonstrating that factors other than gestational diabetes are often associated with an increased rate of macrosomia.15
The ability of plasma glucose (on screening with a 50-g load, while fasting and 2 hours after a 75-g load) to predict birth weight at or above the 90% percentile was investigated by analysis of receiver operating characteristic curves. According to Ouzilleau and colleagues, the predictive value of these 3 plasma glucose variables was “mediocre” and demonstrated “modest risk stratification performance.”
The paper does not mention the proportion of patients who were actually diagnosed with gestational diabetes at the time of their pregnancies. It would appear that the proportion was less than 12.7% or 13.3% (the proportions estimated retrospectively on the basis of ADA criteria, as shown in Table 2 of the paper), given that the diagnostic thresholds used by the institution where the women underwent screening (which were based on National Diabetes Data Group criteria16) were higher than the ADA thresholds. Therefore, it appears that about 90% of the study population had no evidence of gestational diabetes and, for that reason, a high rate of macrosomia should not have been anticipated. Thus, in their conclusions, the investigators are running a risk of type II error.
The results of this carefully conducted study suggest that screening for gestational diabetes in an effort to prevent macrosomia may be unwarranted. This conclusion, however, depends entirely on the authors' assumption that the women identified with gestational diabetes did not undergo any major interventions to lower their glucose intolerance. This may or may not be the case. There is evidence that when patients are identified as having gestational diabetes, they or their physicians may alter their behaviour, which could modify pregnancy outcome.12 For this reason, one must be cautious in interpreting outcomes in this unblinded study, even though only minimal intervention was offered. The researchers went to great lengths to obtain all of the pertinent information, but because the study was retrospective, the management protocol was not standardized, and many actions, interventions or other confounding variables could have been missed. The results should be considered in that light.
The authors did show that progressively increasing glucose values were associated with increasing rate of macrosomia in this predominantly nondiabetic population. The association was thought to be weak and became weaker once other macrosomia-related factors were included in the multivariate analysis. This finding corresponds to the results of the Toronto Tri-Hospital Gestational Diabetes Project.17
This study underscores the controversy at the heart of the debate over the importance, or even the existence, of gestational diabetes. Some physicians in Canada do not believe that this condition exists, and others feel that its importance is so low that screening is not justified.11 Many researchers, in studies like this one, are trying to shed light on this subject,9,17,18 but the controversy will only end once a robust, randomized, double-blind trial is conducted to demonstrate whether identification and management of gestational diabetes is associated with significant improvement in neonatal or maternal outcome. Unfortunately, no such study is yet under way.
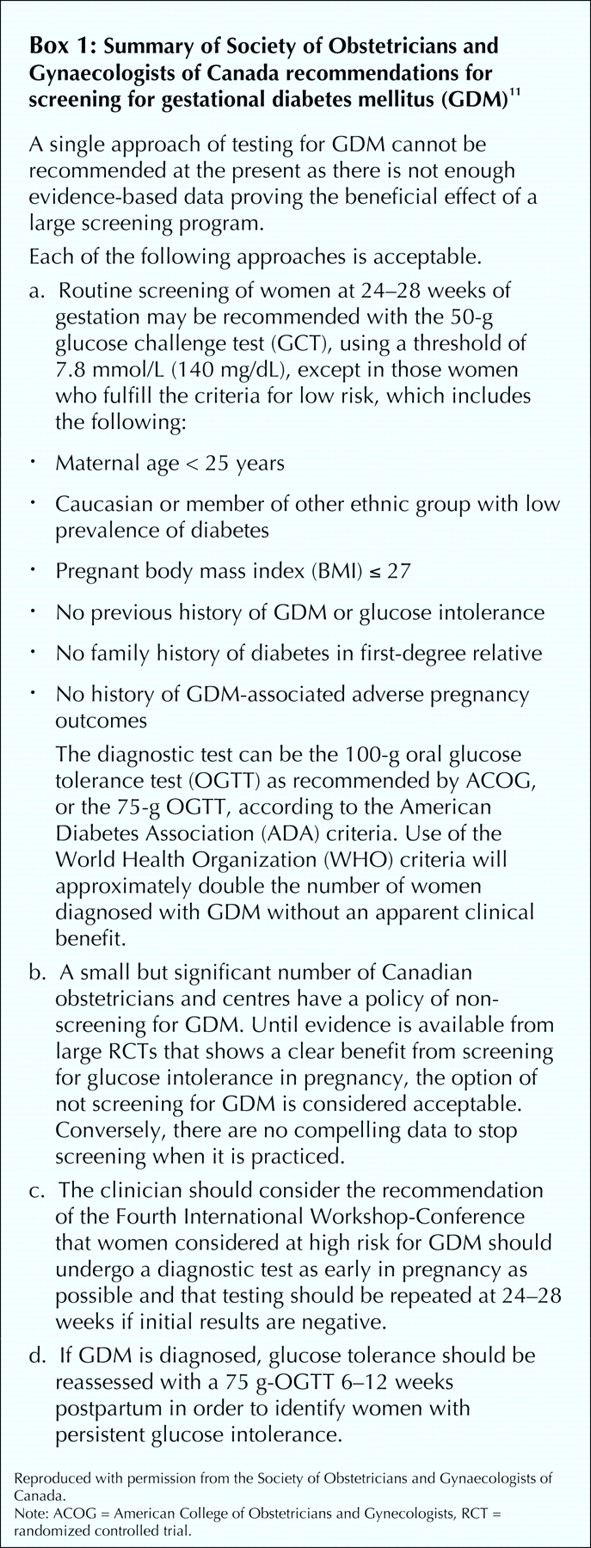
While waiting for the results of such a trial, it would be reasonable to follow the SOGC guidelines published in November 200211 (see Box 1).

{kind=link}
𝛃 See related article page 403
Footnotes
-
Competing interests: None declared.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.