


Abstract
BACKGROUND: Most of the literature on high-cost users of health care has evaluated this population as a whole, but few studies have focused on high-cost patients with mental illness and whether they persist in the high-cost state. We sought to analyze this patient population in depth and determine predictors of persistency in the high-cost state.
METHODS: We used 8 years of longitudinal patient-level population data (2010–2017) from Ontario to follow high-cost patients (those in and above the 90th percentile of the cost distribution) with mental illness. We classified high-cost status, based on the proportion of the study period that patients spent in the high-cost state, as persistent (6–8 yr), sporadic (1–2 yr) or moderate (3–5 yr). We compared characteristics between groups and determined predictors of being a patient with mental illness and persistent high-cost status.
RESULTS: Among 52 638 patients with mental illness and high-cost status, 18 149 (34.5%) were considered persistent high cost. These patients had higher mean annual costs of care ($44 714, 95% confidence interval [CI] $43 724–$45 703) than patients with sporadic ($23 205, 95% CI $22 741–$23 668) and moderate ($31 055, 95% CI $30 359–31 751) status, largely owing to psychiatric hospital admissions. Patients with mental illness and persistent high-cost status were more likely to be female, older, long-term residents of Ontario (information ascertained from the Immigrants, Refugees and Citizenship Canada Database), living in low-income or urban areas, or to have comorbidities. The strongest predictors of persistent (v. sporadic) high-cost status were HIV (relative risk ratio [RRR] 4.32, 95% CI 3.08–6.06), psychosis (RRR 3.41, 95% CI 3.25–3.58) and dementia (RRR 3.21, 95% CI 2.81–3.68).
INTERPRETATION: Among patients with mental illness and high-cost status, persistence in the high-cost state was determined mainly by psychosis and other comorbidities. Quality-of-care interventions directed at managing psychosis and multimorbidity, as well as preventive interventions to target patients with mental illness before they enter the persistent high-cost state, are needed.
To address rising health care costs, it is important to understand the composition of the population of patients with high-cost status. Most work on high-cost patients has considered this population as a whole.1–3 However, previous work has shown that policies and interventions designed to address quality of care and high health care spending in general will likely not apply to all subgroups of high-cost patients.4,5 Moreover, research has shown that high-cost patients are a heterogeneous population.6 For example, high-cost patients who use mainly mental health services are quite different from other high-cost patients — they are younger, live in poorer neighbourhoods and have different patterns of health care use.4,6 They also have high levels of comorbidity and incur over 30% more costs than other high-cost patients, suggesting they may be a more complex population with higher needs.4,6
It is also important to understand whether high-cost patients remain in the high-cost state for long periods of time or whether this is a one-time occurrence. The few studies that have examined persistency in the high-cost state evaluated such patients as a whole and followed them for only 3 years.7,8 Although previous studies have found that individuals with mental illness are more likely to be patients with persistent high-cost status,9,10 no studies have specifically examined persistency in the high-cost state among patients with mental illness4 or followed these patients for long periods of time.11 The goal of this study was to provide an in-depth analysis of patients with mental illness and persistent high-cost status, using administrative health care data from Ontario, Canada’s most populous province.
Methods
Study design and setting
We undertook a retrospective, population-based, longitudinal cohort study of patients with mental illness and high-cost status to examine persistency in the high-cost state from 2010 to 2017, using data from Ontario.
Data
We used administrative health care data available through ICES, in Toronto, to undertake our analysis. The ICES data repository contains individual-level linkable and longitudinal data on most publicly funded health care services for all legal residents of Ontario. It includes several health services databases, many of which have been validated and described in the literature,12 and used in costing analyses.4,6 We used the following databases: Discharge Abstract Database, Ontario Mental Health Reporting System, National Ambulatory Care Reporting System, Ontario Health Insurance Plan claims database, Ontario Drug Benefit claims database, National Rehabilitation Reporting System, Continuing Care Reporting System and Home Care Database. All databases were linked using unique encoded identifiers and analyzed at ICES, in compliance with Ontario privacy legislation. A full description of each database can be found in Appendix 1 (Table A1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.200274/tab-related-content).
Patient cohort
We selected all adult patients (aged 18 yr and older) who had at least 1 encounter with the Ontario health care system in 2010, the index year, and excluded those who did not have a valid health card number. Among these patients, we defined high-cost patients as all patients in and above the 90th percentile of the cost distribution, in line with previous work.4,6,8 This threshold enabled us to select a larger cohort of patients compared with other definitions (e.g., 95th percentile). Patients with mental illness and high-cost status were defined as those for whom costs related to mental health and addiction care accounted for 50% or more of their total costs.4 Previous research has shown that changing the threshold to 60% has little impact on the cohort definition,4 as mental health- and addiction-related costs account for most costs.
Classification of high-cost status for patients with mental illness
Costs related to mental health and addiction care were defined in line with previous work.4 We used a cost estimation algorithm, available at ICES, to estimate all direct health care costs incurred by patients and borne by the Ontario Ministry of Health.13 Details are provided in the appendix. We followed individuals from 2010 to 2017 (i.e., 8 yr) to examine whether they moved in and out of the high-cost state (i.e., above or below the 90th percentile of the cost distribution). Previous work has defined “patients in the persistent (or consistent) high-cost state” as those in the 80th percentile in all 4 half-year periods across 2 years, and “point high-cost patients” as the top users in the first year alone.11 Because this study indicated that patients with persistent high-cost status should incur high costs consistently and continuously over several periods, we defined these patients as those who remained in and above the 90th percentile of the cost distribution for 6 or more years (at any point) over the 8-year study period (i.e., 75% of the analysis period). We defined patients with sporadic high-cost status as those in the high-cost category for 1 or 2 years, and patients with moderate high-cost status as those in the high-cost category for 3, 4 or 5 years. Some patients (the attrition cohort) did not have data for all 8 years, owing to loss to follow-up (e.g., individuals who died, moved out of the province or were no longer eligible for public health care insurance in Ontario). We classified high-cost status similarly in the attrition and nonattrition cohorts and included both in the primary analysis.
Analysis
We compared the 3 patient groups in terms of sociodemographic characteristics — sex, age, migrant status, neighbourhood income quintile, rural residence and administrative health region — and presence of chronic conditions — rheumatoid arthritis, asthma, cancer, chronic obstructive pulmonary disease, diabetes, HIV, hypertension, congestive heart failure, Crohn disease or colitis, myocardial infarction, psychosis and dementia — which were determined through either disease registries (e.g., Ontario Cancer Registry) or validated algorithms.14–25 Given the lack of a validated algorithm to identify other relevant psychiatric chronic conditions, we attempted to determine the presence of mood disorders using at least 1 hospital admission record (with International Classification of Diseases, 10th Revision [ICD-10] codes F30, F31, F32, F33, F34, F38, F39, F53.0 and Diagnostic and Statistical Manual of Mental Disorders, 4th Edition [DSM-IV] codes 296.x, 300.4x, 301.13; all codes correspond to mood and affective disorders) or 2 physician billings (with diagnostic billing code 311 for depressive or other nonpsychotic disorders, not elsewhere classified) within a 1-year period. This algorithm has not been validated; therefore, it was considered only in a sensitivity analysis.
Cost analyses are described in Appendix 1. We undertook a trends analysis of costs over time using linear regression with a time trend for each patient group. We estimated a multinomial logistic regression model26,27 on the pooled data (i.e., all 8 yr of data combined) to determine the predictors of being a patient with mental illness and persistent or moderate high-cost status compared with having sporadic high-cost status, where the dependent variable for each patient was constructed using the previous definitions and its value repeated for each year that patients appeared in the data. This model controlled for the patient sociodemographic characteristics and chronic conditions described above, and calendar year indicators, all of which could vary over the 8 years. We exponentiated the model coefficients to obtain the relative risk ratio for a 1-unit change in the corresponding variable (where risk is measured as the risk of the outcome relative to the base outcome).26,27 We estimated clustered standard errors for all models to account for repeated observations on the same individual, where applicable.
Sensitivity analysis
We undertook sensitivity analyses, where an indicator of mood disorders was included in the model and where patients lost to attrition (i.e., all decedents and individuals ineligible for public health care insurance) were excluded from the analysis. Moreover, we estimated the odds of being a patient with mental illness and persistent high-cost status relative to having moderate and sporadic high-cost status, in line with previous work.8
Ethics approval
This study was approved by the Institutional Review Board at Sunnybrook Health Sciences Centre, Toronto.
Results
Roughly 13% (n = 6975) of individuals from the initial sample (n = 52 638) did not have data for all 8 years of the analysis, owing to loss to follow-up (Table 1). Based on our definitions, 34.5% (n = 18 149) of patients were classified as having persistent high-cost status (18.3% patients were in the high-cost state for all 8 yr), 33.8% (n = 17 746) with sporadic high-cost status and 31.8% (n = 16 743) with moderate.
Years in the high-cost state among patients with mental illness and high-cost status in Ontario, by nonattrition and attrition cohorts (2010–2017)
The overall cohort had a mean age of 45 years and included roughly the same proportion of male (49%) and female (51%) patients (Table 2). Compared with patients with sporadic high-cost status, those with persistent high-cost status were more likely to be older (mean age 47 v. 42 yr) or female (52.7% v. 48.7%); to live in low-income neighbourhoods (30.9% v. 24.6%) or urban areas (93.2% v. 89.7%); and to have psychosis (55.2% v. 31.1%), diabetes (20.9% v. 8.9%), hypertension (30.6% v. 19.8%), chronic obstructive pulmonary disease (15.7% v. 8.1%), dementia (7.2% v. 3.5%) or asthma (22.3% v. 17.3%). Patients with moderate high-cost status were relatively similar to those with persistent high-cost status, except for a lower prevalence of psychosis (40.5% v. 55.2%) and diabetes (13.7% v. 20.9%).
Characteristics of high-cost patients with mental illness in Ontario by high-cost patient group, 2010
Patients with persistent high-cost status had the highest mean costs in 2010 ($44 714, 95% confidence interval [CI] $43 724–$45 703), compared with patients with moderate ($31 055, 95% CI $30 359–$31 751) and sporadic high-cost status ($23 205, 95% CI $22 741–$23 668) (Table 3). In particular, 69% of total costs for patients with persistent high-cost status were made up of costs of psychiatric hospital admissions alone ($30 944, 95% CI $29 956–$31 932), with other large costs incurred by physician services ($5818, 95% CI $5734–$5902), outpatient prescription drugs ($2947, 95% CI $2893–$3000) and visits to hospital outpatient clinics ($2666, 95% CI $2608–$2724). Combined, these costs made up 94.8% of total costs. The proportion of potentially preventable acute-care costs (defined through validated algorithms)28,29,30 was small among all patients with mental illness and high-cost status (0.5% of total costs). Between 2010 and 2017, costs decreased significantly in all 3 groups (p < 0.001) (Figure 1). The average annual decrease in costs was $2935 for patients with moderate high-cost status, $2067 for patients with sporadic high-cost status and $918 for those with persistent high-cost status (p < 0.001 for all between-group comparisons). The appendix provides costs by health service for each year.
Mean health care costs in 2010 for patients with mental illness and high-cost status in Ontario, by high-cost patient group and health service use*
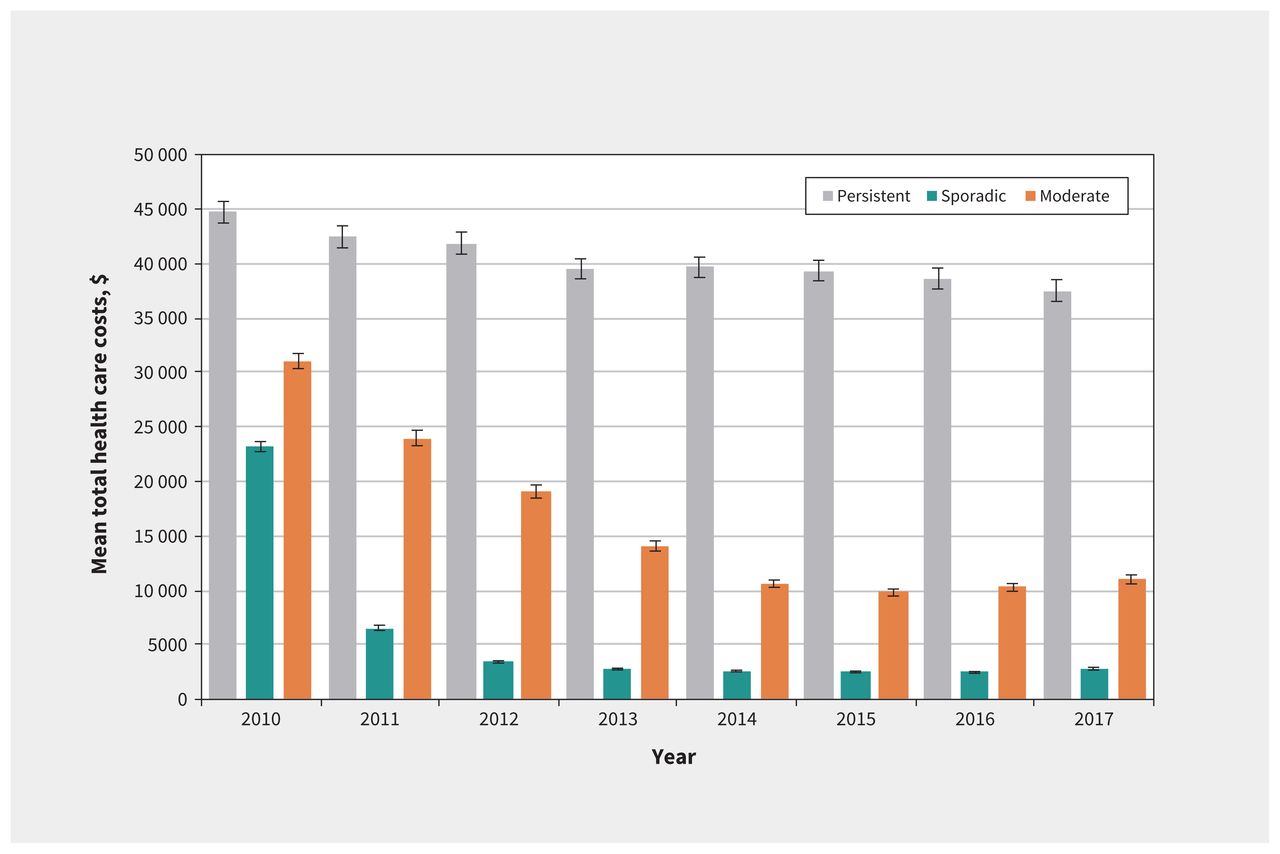
Mean total health care costs for patients with mental illness and high-cost status (n = 52 638) in Ontario by high-cost patient group, 2010–2017. Note: Costs are in 2018 Canadian dollars. Error bars represent 95% confidence intervals. Based on a trends analysis, we found that the average decreases in costs over time were greater for patients with moderate high-cost status ($2935 per year, p < 0.001), followed by sporadic status ($2067 per year, p < 0.001) and persistent high-cost status ($918 per year, p < 0.001); all between-group differences were statistically significant (p < 0.001).
Source: Administrative health care data housed at ICES, Toronto.
The risk of having persistent high-cost status, compared with sporadic high-cost status, was higher for older patients (v. ages 18–44 yr, ages 45–64 yr, relative risk ratio [RRR] 1.19, 95% CI 1.13–1.25; ages 65–84 yr, RRR 1.70, 95% CI 1.52–1.89; ages 85–105 yr, RRR 1.23, 95% CI 0.93–1.62), but lower for men (RRR 0.79, 95% CI 0.75–0.82), immigrants (RRR 0.59, 95% CI 0.53–0.64), refugees (RRR 0.64, 95% CI 0.55–0.74), rural dwellers (RRR 0.61, 95% CI 0.57–0.66) and those living in higher-income neighbourhoods (e.g., highest v. lowest neighbourhood income quintile, RRR 0.84, 95% CI 0.79–0.89) (Table 4). All chronic conditions were associated with increased risk of persistent high-cost status, with the highest relative risk ratios observed for HIV (RRR 4.32, 95% CI 3.08–6.06), psychosis (RRR 3.41, 95% CI 3.25–3.58) and dementia (RRR 3.21, 95% CI 2.81–3.68). Associations of similar or slightly smaller magnitude were found for these variables with the risk of having moderate rather than sporadic high-cost status (Table 4). Appendix 1, Tables A3 and A4, provides the results of the multinomial logistic regressions including mood disorders and excluding patients lost to attrition, respectively; despite minor differences, the main findings were largely unchanged. Appendix 1, Table A5, provides the odds ratios of being a patient with mental illness and persistent high-cost status versus being one with moderate and sporadic status; again, results were qualitatively the same.
Pooled multinomial logistic regression: predictors of persistency in the high-cost state among patients with mental illness and high-cost status (n = 393 511)* in Ontario, 2010–2017
Interpretation
Among our cohort of patients with mental illness and high-cost status, we found that more than 1 in 3 were patients with persistent high-cost status, while nearly 1 in 5 remained in the high-cost state for all 8 years of the analysis. Patients with mental illness and persistent high-cost status were slightly older, slightly more likely to be female, more likely to live in low-income or urban areas and to have psychosis, hypertension, asthma and diabetes, compared with patients with mental illness and with sporadic and moderate high-cost status. Their spending profile also differed — they had higher costs, and the proportion of costs due to psychiatric hospital admissions was larger than those of the other 2 groups. We found that the main predictors of being a patient with mental illness and persistent high-cost status were having HIV, psychosis or dementia. In a sensitivity analysis, we also found that having a mood disorder was predictive of being a patient with mental illness and persistent high-cost status. Results were largely unchanged when we dropped individuals who were lost to attrition over time. It is not surprising that having psychosis is predictive of being this kind of patient; previous research has found that patients with psychosis have high costs of care.31 Moreover, having diabetes was also an important predictor of persistent high-cost status. Other work has found that individuals with psychosis are less likely to have optimal diabetes care than those without psychosis, resulting in higher rates of diabetes-related hospital admissions, 32 which can lead to higher costs.
Few studies have examined persistency in the high-cost state, particularly among patients with mental illness. Using administrative data from Ontario, Wodchis and colleagues found that 30.7% of individuals in the top 5% remained in the high-cost state from 2009 to 2011.7 Figueroa and colleagues examined persistency in the high-cost state among a 20% sample of Medicare fee-for-service beneficiaries from 2012 to 2014 in the United States, using data on inpatient and outpatient care, physician services, tests and procedures, and drugs.8 They found that 28.1% of high-cost patients in the top 10% remained in the high-cost state for all 3 years. These patients were younger and more likely to be individuals of colour, live in lower-income areas, be Medicare eligible, and be dually eligible for Medicare and Medicaid compared with transient- and never-high-cost patients. Furthermore, they found that the spending of patients with persistent high-cost status was mostly due to outpatient care and drugs. Although we examined a subgroup of patients with high-cost status, we also found that more patients with mental illness and persistent high-cost status lived in lower-income areas than patients with mental illness and moderate and sporadic high-cost status. However, these patients’ spending profile was substantially different — most costs were due to psychiatric hospital admissions, further confirming the need to consider them separately from other high-cost patients. In line with Figueroa and colleagues, we also found that a small proportion of spending was due to preventable acute-care hospital admissions among patients with mental illness and high-cost status. This is not surprising as most costs were due to psychiatric hospital admissions and not acute-care admissions. Therefore, it may make more sense to try to ascertain preventable psychiatric hospital admissions, where possible. Although some psychiatric hospital admissions are likely part of the natural course of the disease, and thus inevitable, some admissions to hospital, namely readmissions, could potentially be prevented through timely access to physician care33 and adherence to medication.34 This should be explored in future research. Also, as a nontrivial number of patients persisted in the high-cost state for 8 years, models predicting long-term persistency may also prove useful for decision-makers. This may require a better understanding of how to prevent multimorbidity from developing among individuals with severe mental illness; for example, through screening of chronic conditions where appropriate.35
We examined all adult patients with mental illness and high-cost status in Ontario; previous work has typically examined representative samples or patients aged 65 years and older only. We followed patients for 8 years; most related work has followed patients for 3 years. Finally, we captured most health care services paid by the Ontario Ministry of Health. Although there is a large body of work on all patients with high-cost status,9,36,37 little attention has been devoted to those with mental illness or examined their trajectories of care.4 At a health-systems level, this research will help inform interventions that preserve quality of care while reducing costs, including preventing persistence in the high-cost state. Previous literature suggests that patients with persistent high-cost status may be an ideal focus for cost-saving interventions, as some costs may be reduced through proper disease management. 28 For example, high support housing38 may help address long hospital stays, which are a driver of high costs. However, our results suggest there may be little scope to address these patients’ high costs without further understanding the reasons for high hospital admission costs and for related outcomes such as long lengths of stay in hospital. These findings may be useful to inform initiatives that focus on improving the management of care among complex, high-need patients with medical and psychiatric multi-morbidity, such as the Health Links Initiative in Ontario,39 Accountable Care Organizations5 in the US and the Better Care Fund40 in the United Kingdom.40
Limitations
We did not examine children and adolescents, as some health services for this population are funded by ministries other than the Ministry of Health. We could not capture patients who did not access the health care system via settings for which we did not have data. For example, we were not able to include the costs of community-based addiction-related care. We were able to capture only costs of outpatient drugs covered by the public provincial drug plan (although this was in line with the perspective of the analysis). The lack of these costs may have affected how patient cohorts were determined. Furthermore, we were able to examine only chronic conditions for which there were validated algorithms. This was particularly problematic for psychiatric conditions as there is a validated algorithm only for psychosis (the mood disorders algorithm is not validated and its definition was limited to the quality of the Ontario physician billings data; moreover, it likely underestimates the number of patients with mood disorders). Additionally, because of data limitations, we were not able to characterize patients in terms of their ethnicity or race, as was done in previous research.5
Conclusion
Many patients with mental illness and high-cost status persisted in the high-cost state, particularly those in low-income or urban areas and with comorbidities. The higher costs incurred by this group were driven by psychiatric hospital admissions. Policymakers should consider interventions that address quality of care through the management of psychosis and multimorbidity and high health care costs, as well as appropriate prevention policies aimed at patients with mental illness before they enter the persistent high-cost state. More research is required to understand what more can be done to address persistency in the high-cost state and whether there may be potential to reduce psychiatric hospital admission or the length of hospital stays.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Claire de Oliveira conceived and designed the work; contributed to the acquisition, analysis and interpretation of data; and drafted the manuscript. Joyce Mason and Paul Kurdyak contributed to the acquisition, analysis and interpretation of data. All of the authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data sharing: The data from this study are held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS.
Disclaimer: This research was funded by the Canadian Institutes of Health Research (CIHR) and supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from funding sources. No endorsement by CIHR, ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of CIHI.
- Accepted August 6, 2020.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

