


In 2009, Health Canada’s Food Directorate received a submission from industry requesting approval to use a claim of reduced disease risk on labels of vegetable oils and foods containing vegetable oils.1 The health claim was related to the replacement of saturated animal fats with unsaturated fats, including polyunsaturated fatty acids, for “a reduced risk of heart disease by lowering blood cholesterol levels.”1 Health Canada’s Food Directorate reviewed the available published literature and concluded that, when saturated fats were replaced with polyunsaturated fatty acids, there was a statistically significant reduction in total and low-density lipoprotein (LDL) cholesterol, that the result was a reduction in the risk of coronary artery disease and that the therapeutic health claim (Box 1) was substantiated by scientific evidence and therefore was valid and “relevant to the Canadian population,” given nearly half of Canadians have hyperlipidemia.1
The following statements can be made in the labelling and advertising of food products that meet the qualifying criteria1
Primary statement:
“Replacing saturated fats with polyunsaturated and monounsaturated fats (from vegetable oils) helps lower/reduce cholesterol. [Statement that the food is reduced or lower in saturated fat as defined in items 20 and 21, respectively, in the table following section B.01.513 of the Food and Drug Regulations] (and is a source of omega-3/omega-6 polyunsaturated fat).”
Examples:
If the food is a vegetable oil:
“Replacing saturated fats with polyunsaturated and monounsaturated fats from vegetable oils helps lower cholesterol. 2 teaspoons (10 mL) of this blend of corn and canola oil contains 84% less saturated fat than 2 teaspoons (10 g) of butter.”
If the food is made with a vegetable oil or a blend of vegetable oils:
“Replacing saturated fats with polyunsaturated and monounsaturated fats from vegetable oils helps lower cholesterol. This blueberry muffin (55 g) is made with canola oil, contains 25% less saturated fat than our regular blueberry muffin (60 g) and is a source of omega-3 polyunsaturated fat.”
The following additional statement could be used in letters up to the same size and prominence as those of the primary statement:
“High cholesterol is a risk factor for heart disease.”
Careful evaluation of recent evidence, however, suggests that allowing a health claim for vegetable oils rich in omega-6 linoleic acid but relatively poor in omega-3 α-linolenic acid may not be warranted (Table 1).2–6
Summary of common sources of evidence relating omega-6 linoleic acid or a mixture of linoleic and omega-3 α-linolenic acids to cardiovascular health benefits
What is known about the cardiovascular health benefits of polyunsaturated fatty acids?
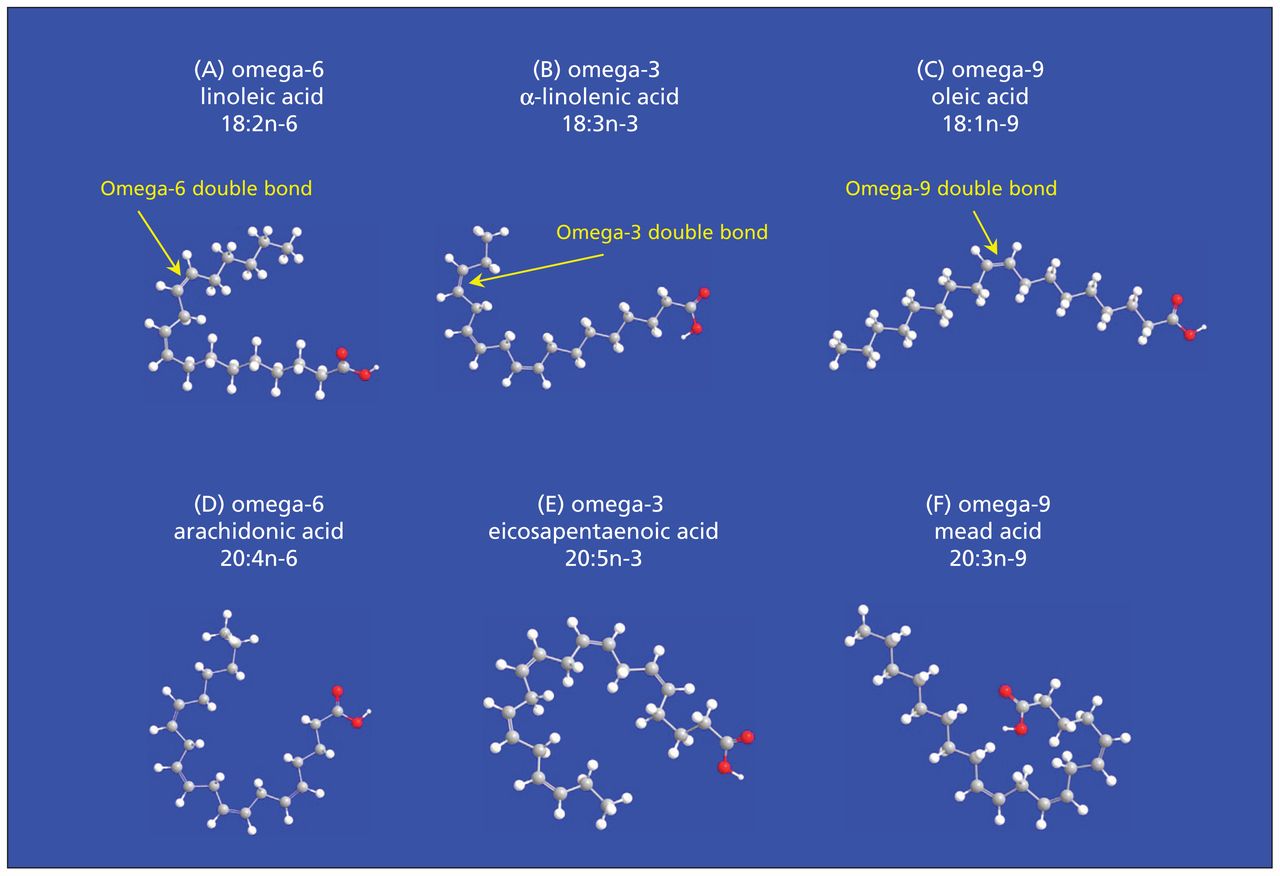
Polyunsaturated fatty acids are fatty acids with 2 or more double bonds in the carbon chain. The most nutritionally relevant are the omega-3 fatty acids (α-linolenic acid, eicosapentaenoic acid and docosahexaenoic acid) and the omega-6 fatty acids (linoleic acid, γ-linolenic acid and arachidonic acid) (Figure 1, Table 2). The health claim refers to polyunsaturated fatty acids derived from vegetable oils, largely omega-6 linoleic acid and omega-3 α-linolenic acid, and not to those derived from fish oils, such as eicosapentaenoic acid and docosahexaenoic acid (Figure 1, Table 2). Several large randomized controlled trials have shown fish oils to be associated with a decreased risk of cardiovascular events.7,8 However, LDL and total cholesterol levels were either increased7 or not different from those in controls,8 which may explain why omega-3 fatty acids from fish oils are exempt from the cholesterol-lowering health claim.

The structure of selected unsaturated fatty acids. (A) Linoleic acid (18:2n-6) is 18 carbons long with 2 double bonds. It is in the omega-6 family of fatty acids because the first double bond is on the sixth carbon from the methyl terminal end. (B) α-Linolenic acid (18:3n-3) is also 18 carbons long, but with 3 double bonds. It is in the omega-3 family because the first double bond is on the third carbon from the methyl terminal end. Both omega-6 and omega-3 fatty acids cannot be synthesized de novo in mammals and therefore are considered nutritionally essential. (C) Oleic acid is an omega-9 fatty acid that can be obtained from the diet or synthesized de novo. (D) Arachidonic acid is an omega-6 fatty acid that can be obtained from the diet or from the metabolism of linoleic acid. (E) Eicosapentaenoic acid is an omega-3 fatty acid that can be synthesized from α-linolenic acid or obtained from the diet, especially from fish oils. Although the term “polyunsaturated fatty acid” generally refers to the omega-6 and omega-3 families, mead acid (F) is technically an omega-9 polyunsaturated fatty acid. Some confusion arises because linoleic acid is quantitatively the most abundant dietary omega-6 polyunsaturated fatty acid, and thus the terms “linoleic acid” and “omega-6 polyunsaturated fatty acid” or even “polyunsaturated fatty acids” are sometimes used interchangeably. Furthermore, chemists commonly number carbons from the carboxylic acid (red) end, whereas nutritionists number them from the omega (methyl) end.
Selected polyunsaturated fatty acids
Neither omega-3 nor omega-6 fatty acids can be synthesized de novo in mammals and are considered nutritionally essential.9,10 The nutritional requirement of linoleic acid is not fully agreed upon, possibly because most of the animal modelling and human cases of linoleic acid deficiency were not specific to linoleic acid and included the deficiency of multiple fatty acids, sometimes referred to as essential fatty acid deficiency.11 The nutritional requirement of linoleic acid has been estimated to be as high as 2% of energy but is likely closer to 0.4% of energy.11 Nevertheless, the current dietary intake of linoleic acid by Canadians is about 5%–6% of energy, and Health Canada reports no concerns regarding low intake levels of linoleic acid in Canada.12 Whereas the US Institute of Medicine has determined adequate intakes for both linoleic acid and α-linolenic acid, there are no formal requirements for eicosapentaenoic acid or docosahexaenoic acid,9 in part because they can be synthesized from α-linolenic acid.9,10 As with linoleic acid, intakes of α-linolenic acid in Canada are generally considered to be adequate.12
What high-quality evidence supports the health claim?
Consistent with the health claim, a 2003 meta-analysis supported the finding that substitution of saturated fatty acids with vegetable oils rich in polyunsaturated fatty acids, including linoleic acid, lowers serum total and LDL cholesterol levels.2 However, the effect of this substitution on the risk of coronary artery disease is not clear. In 2010, a meta-analysis of clinical trials, cited by Health Canada’s Food Directorate,1 reported that substituting vegetable oils rich in polyunsaturated fatty acids for saturated fat lowers the risk of coronary artery disease (risk ratio [RR] 0.90, 95% confidence interval [CI] 0.83–0.97, for each change of 5% energy).13 The American Heart Association and the media14 have ascribed the noted beneficial effects to linoleic acid, at least in part.15 The American Heart Association stated that “higher intakes [of linoleic acid] appear to be safe and may be even more beneficial (as part of a low–saturated-fat, low-cholesterol diet).”15 This recommendation is shared by some, but not all, nutritional guidelines.16
A closer look at the composition of the vegetable oils used in the individual clinical trials raises doubt as to whether the protective effects can be attributed to linoleic acid. In 2010, Ramsden and colleagues performed a detailed analysis of the sources and fatty-acid composition of dietary fats that were exchanged in the clinical trials.17 They noted that rates of nonfatal myocardial infarction and death from coronary artery disease were 22% lower (RR 0.78, 95% CI 0.65–0.93) when oils containing a mix of linoleic and omega-3 fatty acids were substituted. However, the rates of nonfatal myocardial infarction and death from coronary artery disease were not significantly lower (RR 1.13, 95% CI 0.84–1.53) when oils made up mostly of linoleic acid but relatively low in α-linolenic acid were substituted. As discussed by Ramsden and colleagues and others,17,18 it seems unlikely that the beneficial effects of vegetable oils can be attributed to linoleic acid.
Soybean oil (mixed linoleic and α-linolenic acids; Table 3) was the most commonly substituted oil in the collective group of studies that showed a protective effect. Corn and safflower oil (oils rich in linoleic acid; Table 3), which contain virtually no α-linolenic acid, were not associated with a benefit. A test of heterogeneity between oils rich in linoleic acid and those containing mixed polyunsaturated fatty acids was statistically different for nonfatal myocardial infarction and death from coronary artery disease (p = 0.02).17 This finding supports the idea that oils rich in linoleic acid should not be grouped with those containing mixed polyunsaturated fatty acids. However, because relatively few studies examined linoleic acid specifically (3 clinical trials),17 it is not possible to draw strong conclusions.
Composition of common vegetable oils
Ramsden and colleagues recently completed a detailed reanalysis of recovered data from the Sydney Diet Heart Study, in which the intervention group replaced saturated fat with sources of safflower oil or safflower oil margarine (rich in omega-6 linoleic acid but low in omega-3 α-linoleic acid).5 They found that the intervention group had serum cholesterol levels that were significantly decreased (by about 8%–13%) relative to baseline and the control group, which is consistent with the health claim. However, the intervention group had significantly higher rates of death than the control group (all cause 17.6% v. 11.8% [hazard ratio (HR) 1.62, 95% CI 1.00–2.64]; cardiovascular disease 17.2% v. 11.0% [HR 1.70, 95% CI 1.03–2.80]; and coronary artery disease 16.3% v. 10.1% [HR 1.74, 95% CI 1.04–2.92]).
After updating their previous meta-analysis with the recovered data, Ramsden and colleagues reported that the rate of death from coronary artery disease was not significantly lower when saturated fats were replaced with oils containing mixed polyunsaturated fatty acids (HR 0.81, 95% CI 0.64–1.03); however, the rate of cardiovascular-related death was significantly reduced (HR 0.79, 95% CI 0.63–0.99).5 They also confirmed that the use of oils rich in linoleic acid was not associated with a significant decrease in death from coronary artery disease (HR 1.33, 95% CI 0.99–1.79) or from cardiovascular disease (HR 1.27, 95% CI 0.98–1.65). Although the mechanism by which replacing saturated fats with omega-6 linoleic acid would increase the risk of death from coronary artery disease is unclear, the authors noted that oxidized linoleic acid is the most abundant oxidized fatty acid in lipoproteins. Secondary analyses confirmed that the detrimental effects of linoleic acid were seen in participants who were smokers and those who consumed alcohol, people likely to be under increased oxidative stress.
The re-evaluation of data from the Sydney Diet Heart Study had limitations.5 The participants were survivors of a recent coronary event, about 70% were smokers, and the study may have been underpowered. Furthermore, the exact composition of fatty acids in the substitute margarine was not known, and it may have included trans fatty acids. However, the intervention resulted in decreased serum cholesterol levels, and the effects remained significant after theoretical adjustments for trans fatty acids. The updated meta-analysis also had limitations.5 Several of the clinical trials involved patients with psychiatric disorders or with existing coronary artery disease. Furthermore, multiple fats were replaced in the control groups, and different doses and sources of oils were used in the intervention groups.
Notwithstanding these limitations, Ramsden and colleagues’ reanalysis has raised several important questions. Is it fair to say that there was a trend toward omega-6 linoleic acid increasing the risk of death from coronary artery disease when the 95% CI in the meta-analysis was 0.99–1.79, overlapping 1? Should oils that are rich in omega-6 linoleic acid and that lower cholesterol be granted a health claim that implies a reduction in risk of coronary artery disease based on these data? Was it the omega-3 α-linolenic acid in the oils with mixed polyunsaturated fatty acids that was protective against death from cardiovascular disease? Despite the limitations of recent studies, it seems unlikely, however, that additional secondary analyses or new interpretations of these datasets will lead to the conclusion that increasing intake of omega-6 linoleic acid will decrease the risk of death from coronary artery disease.
What have epidemiologic studies shown?
When considering evidence for the health claim, inclusion of prospective cohort studies that have examined omega-6 linoleic acid and coronary artery disease is probably warranted given the limitations of the clinical trials. A summary of the evidence provided from prospective cohort studies is shown in Table 1.
In observational studies, foods are usually identified and quantified using a food frequency questionnaire and are matched to databases with the nutrient composition of the foods. The assessment of dietary intakes of omega-6 linoleic acid and omega-3 α-linolenic acid from food frequency questionnaires has been criticized.6 In addition, dietary intake of α-linolenic acid as measured by food frequency questionnaires has been found to correlate weakly with plasma phospholipid, cholesteryl ester and adipose levels (Pearson correlation coefficients 0.15 and 0.31, and Spearman correlation coefficient 0.33, respectively; p < 0.05) in some food frequency questionnaires,21,22 and to have no significant correlation with adipose, erythrocyte or plasma α-linolenic acid levels (Spearman correlation coefficients 0.01–0.12 for adipose and 0.17–0.23 for blood measures; p > 0.05) in other food frequency questionnaires.21,23 However, dietary intake of both linoleic and α-linolenic acids as measured by food frequency questionnaires correlate moderately with each other (Spearman correlation coefficient 0.49, p < 0.001).24 Thus, it is unclear whether the methodologic features of food frequency questionnaires can isolate dietary linoleic acid from α-linolenic acid.
Dietary sources of omega-6 linoleic acid measured by food frequency questionnaires are not reported in most prospective studies examining coronary artery disease. In one report from the Nurses Health Cohort, in which increasing intake of linoleic acid was associated with an increased risk of clinical depression,25 separately published food sources of linoleic acid26 were mayonnaise or other creamy vinaigrettes (14.6% of total dietary linoleic acid), margarine (9.8%), oil and vinegar salad dressing (9.1%), fried food at home and away (7.1%), chips (5.5%), nuts (4.7%) and peanut butter (4.1%).26 It is unclear whether any of these foods were associated with the protective effects against coronary artery disease ascribed to linoleic acid observed in some,3 but not all,4 of the prospective cohorts.
What are the trends in oil usage in Canada?
Currently, relatively pure dietary oil sources of omega-6 linoleic acid make up only 5% of oils in the Canadian diet; canola oil and soybean oil account for about 55% and 25% of dietary intake, respectively,27 both of which contain mixed linoleic and α-linolenic acids (Table 3). An emerging body of literature supports the hypothesis that omega-3 α-linolenic acid may reduce the risk of coronary artery disease,28 but evidence from clinical trials that have attempted to isolate α-linolenic acid is limited.29 In Canada and elsewhere, traditional canola and soybean oils are being replaced with versions high in oleic acid (an omega-9 monounsaturated fatty acid), at the expense of omega-6 linoleic acid and especially omega-3 α-linolenic acid. The effect of oils high in oleic acid on the risk of cardiovascular disease has yet to be tested in randomized or prospective trials.
Conclusion
In summary, much confusion has arisen from unclear nomenclature with regard to polyunsaturated fatty acids and the lack of reporting of food sources in prospective cohorts. Data from prospective cohort studies and randomized controlled trials generally support the replacement of saturated fats with mixed polyunsaturated fatty acids to reduce the risk of death from coronary artery disease. However, it is unclear whether oils rich in omega-6 linoleic acid but low in omega-3 α-linolenic acid also reduce this risk. We suggest that the health claim be modified such that foods rich in omega-6 linoleic acid but poor in omega-3 α-linolenic acid be excluded. Future research is needed to examine the dietary methodologies used to measure polyunsaturated fatty acid intakes in observational studies and the metabolism of polyunsaturated fatty acids, as well as their role in coronary artery disease and other diseases.
Key pointsThe replacement of dietary saturated fats with some, but not all polyunsaturated fatty acids reduces serum cholesterol levels and the risk of heart disease.
New analyses suggest that replacing saturated animal fats with linoleic acid, an omega-6 polyunsaturated fatty acid, lowers serum cholesterol levels but increases the risk of death from coronary artery disease.
Health Canada’s Food Directorate should reconsider the health claim that omega-6 polyunsaturated fatty acids reduce the risk of heart disease by lowering blood cholesterol levels.
Footnotes
Competing interests: Richard Bazinet has received research funding from Bunge Ltd., travel support from Unilever and consultant fees from Kraft Foods Inc. Michael Chu has received speaker fees and laboratory research support from Medtronic of Canada Ltd. and Edwards Lifesciences; he has also received laboratory research support from NeoChord Inc.
This article has been peer reviewed.
Contributors: Both authors were responsible for the conception and design of the article, and the collection, analysis and interpretation of the data. Both of the authors drafted the manuscript, revised it for important intellectual content and approved the final version submitted for publication.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

