


Abstract
Background: Group medical visits, whereby health care professionals meet with groups of patients who have the same disease, have been introduced in primary care as a way to meet the increasing demand for health care delivery to patients with chronic diseases. We performed a systematic review and meta-analysis of the evidence on the effectiveness of such visits for patients with diabetes.
Methods: We conducted a systematic review of all relevant studies published from 1947 to February 2012 identified in a search of electronic databases and grey literature. We included randomized controlled trials (RCTs) and observational studies published in English that included patients aged 16–80 years with type 1 or 2 diabetes and that had group medical visits as the intervention. These studies were assessed for methodologic quality. We included data only from the RCTs in the meta-analysis.
Results: Of the 94 studies identified, we selected 26 that met our inclusion criteria, 13 of which were RCTs. Group medical visits had a positive effect on clinical and patient-reported outcomes, with significant reductions in glycated hemoglobin (HbA1c reduction −0.46%, 95% confidence interval −0.80% to −0.31%). We were unable to assess the effect of group medical visits on processes of care because of an insufficient number of RCTs that reported on this outcome.
Interpretation: Group medical visits for patients with diabetes were found to be effective in terms of reducing HbA1c. The results of our meta-analysis suggest that wider implementation of group medical visits for patients with diabetes will have a positive effect on patient outcomes.
Increasing evidence shows that strengthening the foundation of primary health care will lead to improved health and provide better management for people with one or more chronic conditions.1 In Canada, increased attention on the primary health care system is particularly important given the growing number of people living with one or more chronic conditions.2 The move to renew and redesign primary care has led to a number of innovations, including group medical visits.3
Group medical visits are a format for health care delivery whereby medical appointments are offered to a group of patients with the same disease instead of the traditional one-to-one patient–provider format.4 During the group visit, patients receive a health evaluation and educational information about their condition and about the prevention of complications and disease progression, and they may have prescriptions, referrals and laboratory tests ordered. The visit is usually facilitated by a physician or a nurse practitioner and may involve other interdisciplinary team members such as a registered nurse, nutritionist and pharmacist.5
Group medical visits offer an ideal format for patients with chronic diseases because they allow health care practitioners to provide care to 12–15 patients in one appointment and enable patients to interact with people who share their condition. In Canada, group medical visits are increasingly being used to provide primary health care to patients with diabetes.3 Type 1 and type 2 diabetes affect about 6.8% of the Canadian population.6 Social support from peers with diabetes has been shown to improve some clinical outcomes.7,8
Although health care providers have reported this care model to be an effective way to deliver care,9–12 data are limited and differ on the impact of group medical visits on patient outcomes. We conducted a systematic review and meta-analysis to measure the effect of group medical visits on biophysical, process-of-care and patient-reported outcomes among patients with type 1 and 2 diabetes.
Methods
We used the PICO (population, intervention, comparison and outcome) approach to develop the research question for our systematic review — population: patients with type 1 or 2 diabetes; intervention: group medical visits; comparison: usual care; outcomes: biophysical, patient-reported and process-of-care outcomes.
Literature search
We conducted a comprehensive search of the following electronic databases from inception through February 2012: MEDLINE (PubMed), CINAHL, Biosis, ProQuest Dissertations and Theses, Embase, Web of Science, Psych Info and the Cochrane Database of Systematic Reviews. We also searched various sources of grey literature. Bibliographies of selected articles were manually searched for additional studies. Details of our search strategies are available in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130053/-/DC1). A librarian was consulted to review the search strategy.
Study selection
A 3-step process was used to determine the eligibility of studies for our review. First, the title of relevant articles were independently screened by each of us. Second, if titles were deemed relevant, abstracts were independently reviewed by 2 of us (L.H. and either S.T.W. or M.D.). Finally, if abstracts were deemed relevant, full-text articles were independently reviewed by 2 of us (as described above). Decisions regarding inclusion and exclusion of studies were made by consensus between the 2 reviewers; disagreements were resolved by the third reviewer as required.
We included randomized controlled trials (RCTs) and observational studies published in English or translated into English that included patients aged 16–80 years with type 1 or 2 diabetes and had group medical visits as the intervention. We excluded studies in which the intervention was for educational purposes or did not include a health care provider who could diagnose, prescribe, make referrals and order laboratory tests.
Multiple articles from the same study or group of patients were classified as “kinned” articles. We grouped kinned articles together and counted them as one study.
Data extraction
We collected data on study characteristics, participant demographics, and clinical and patient-reported outcomes. Where possible, sample size and post-intervention means and standard deviations (SDs) were extracted for both the intervention and usual-care groups. We extracted data from the observational studies to inform the discussion. Data were initially extracted by one of us (L.H.) and checked by the others (S.T.W., M.D.) to ensure accuracy.
Assessment of bias
We assessed RCTs for risk of bias using the Cochrane Risk of Bias Tool.13 One of us (L.H.) completed the full quality assessment. Congruency of the assessment was ensured by having a second reviewer (S.T.W.) independently assess quality of 5% of the included studies. A sensitivity analysis was performed in which we excluded studies that had 2 or more items with a high risk of bias. Because some articles included patients with either type 1 or type 2 diabetes, we conducted an additional sensitivity analysis for glycated hemoglobin (HbA1c) in which we excluded studies that included only patients with type 1 diabetes as well as studies in which the type of diabetes was unclear. Overall effect size, significance and funnel plots were examined for HbA1c.
Data synthesis
We included only RCTs in the meta-analysis. We analyzed the data from RCTs using Review Manager software (RevMan, version 5.1, Nordic Cochrane Centre). For each RCT, the effect size was calculated to determine the mean differences between the intervention and control groups at the longest reported time after the intervention.
Mean differences were first pooled into a fixed-effects model. A χ2 test for heterogeneity was performed; when significant heterogeneity was found (I2 > 25%), the analysis was recalculated with a random-effects model. The mean differences were weighted and pooled following Hedges’ method for calculating standardized mean differences.14
When measures of dispersion were not reported for outcome data, we used baseline SDs or calculated SDs from reported p values. When no baseline SD or p values were reported, we estimated SDs from the baseline range data. When examining these estimated SDs, we found that they were conservative estimates of the value; a sensitivity analysis in which we removed studies with uncertain SDs yielded improved HbA1c outomes with a decrease in effect size.
We performed a meta-regression analysis to determine (a) if the length of time patients spent attending group medical visits was related to effect size and (b) if the number of group visits a patient attended in a year was related to effect size. To examine the number of group visits attended per year, we created an “intensity” value by dividing the number of appointments by the number of years of the intervention. For the meta-regression analysis, we used Stata software, version 12.1 (StataCorp LP).
Results
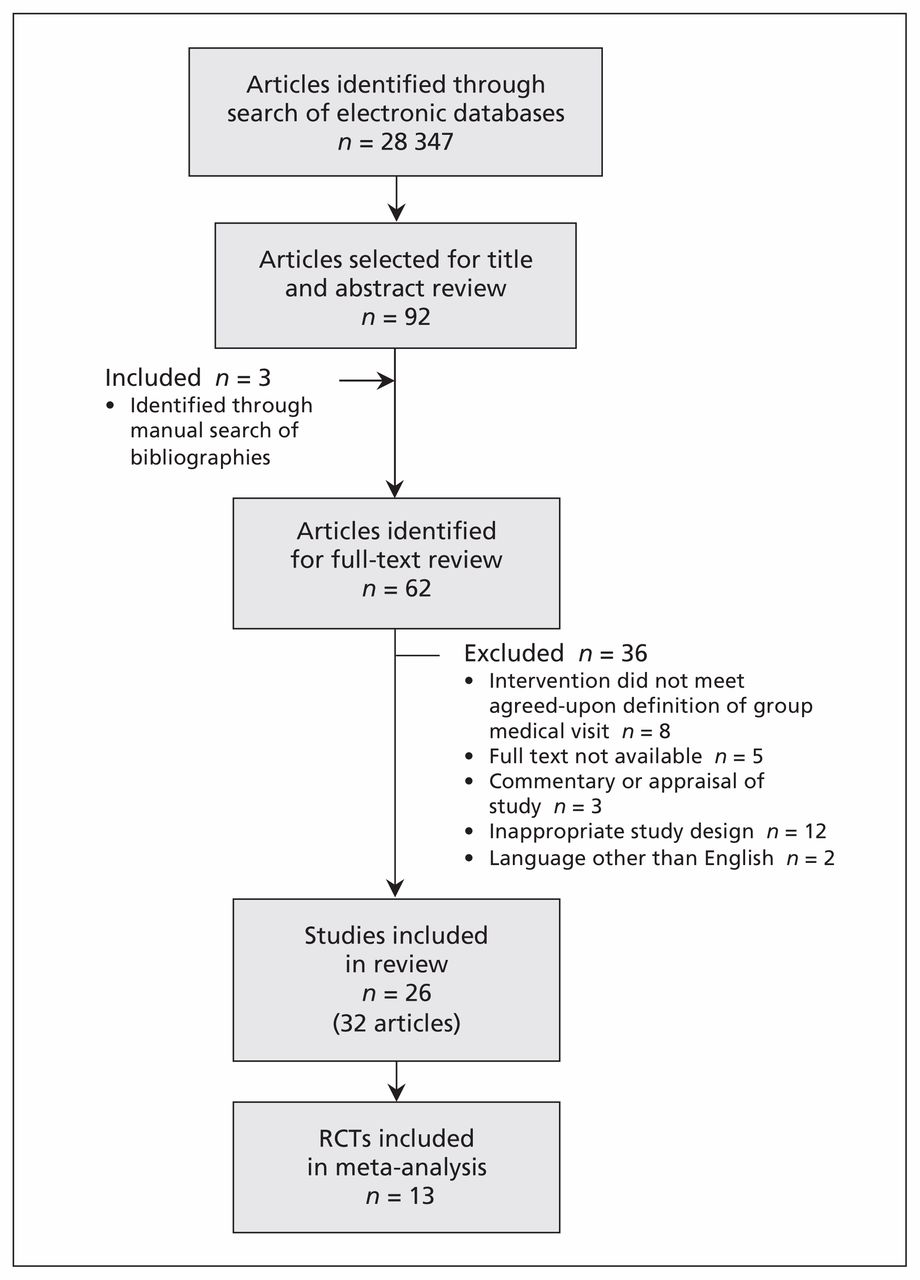
We identified 92 potentially eligible articles. The most common reasons for exclusion were that the intervention did not involve a health care provider who could prescribe, diagnose, assess and refer patients; the article was a narrative or commentary based on other research studies; the study did not include a group medical visit as the intervention; and the article was not in English. A total of 26 studies met our inclusion criteria (Figure 1).5,15–45

Selection of studies. RCT = randomized controlled trial.
Study characteristics
The characteristics of the 13 RCTs included in the meta-analysis are summarized in Table 115–33 (for characteristics of all 26 studies, see Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130053/-/DC1). The number of studies published after 2002 increased substantially (4 studies before 2002, 12 between 2002 and 2007, and 16 between 2008 and 2012). One document was a doctoral dissertation, completed in 2011.43 Most of the studies (n = 20) were conducted in the United States,5,15–23,25–28,33,34,36–43 with the remainder conducted in Europe (Austria n = 1,44 France n = 1,35 Italy n = 329–32,45 Norway n = 124). Samples ranged in size from 37 to 707 participants. Three studies included fewer than 50 patients, and 6 had more than 200; the remainder had between 50 and 100 patients (n = 7 studies) or between 100 and 200 patients (n = 10).
Characteristics of 13 randomized controlled trials included in the meta-analysis
Of the total 4652 patients, 3112 received group care or attended group medical visits as an intervention. The mean age of participants in the studies that reported this information was 59.3 years, and 56% of participants attending group medical visits were men.
Study quality
A summary of the risk-of-bias assessment of the 13 RCTs can be found in Table 2. The amount of bias varied across the trials. Only one had a low risk of bias in most areas.22 The other RCTs either did not report enough information for bias to be assessed or had 2 or more areas assessed as a high source of bias.
Risk-of-bias assessment of the randomized controlled trials
Clinical outcomes
Eleven of the RCTs reported HbA1c data at baseline. The baseline values did not differ significantly between the studies (weighted mean difference −0.09, 95% confidence interval [CI] −0.29 to 0.11). Only 10 studies reported HbA1c data that could be included in our meta-analysis. Pooled analysis of HbA1c values after the intervention period showed significantly lower values among the patients attending group medical visits (weighted mean difference −0.46, 95% CI −0.80 to −0.13) (Table 3, Figure 2).
Pooled analysis of the effect of group medical visits on clinical outcomes reported in randomized controlled trials

Pooled analysis of the effect of group medical visits versus usual care for patients with diabetes on glycated hemoglobin (HbA1c) reported in randomized controlled trials. A weighted mean difference of less than zero indicates a positive effect of group medical visits. CI = confidence interval, SD = standard deviation.
In the meta-regression analysis, we found that duration of treatment directly affected patients’ HbA1c values. Patients who attended group medical visits for longer periods had better HbA1c outcomes. For every year increase in the duration of treatment, there was a decrease in effect size of 0.25, which indicated a drop in HbA1c of one quarter of 1%. When we examined whether the frequency of group visits had an effect on HbA1c outcomes, it did not explain the difference in the effect size, which indicated that the duration of treatment had a greater effect on HbA1c outcomes than the number of appointments attended per year. We did not analyze other attributes of group visits using meta-regression techniques because the data were not consistently reported in the RCTs.
When we excluded studies with 2 or more methodologic features assessed as a high source of bias, the overall effect of group medical visits on HbA1c improved (weighted mean difference −0.62, 95% CI −1.23 to −0.01). When we excluded studies with 3 or more features assessed as a high source of bias, the effect size did not change significantly (−0.47, 95% CI −0.94 to 0.00). When we excluded studies that had only patients with type 1 diabetes, the effect size increased (−0.58, 95% CI −1.12 to −0.04).
Five of the RCTs evaluated the effects of group medical visits on systolic blood pressure, and 4 assessed the effects on diastolic pressure. No statistically significant effect on either type of blood pressure was found in the meta-analysis (Table 3; see also Appendix 3, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130053/-/DC1).
Group medical visits had a slightly positive effect on patients’ weight, but no effect on body mass index; the effect on weight was not statistically significant. A negative effect of group medical visits on total and high-density lipoprotein cholesterol levels was noted; however, the effects were minimal (Table 3, Appendix 3).
Other outcomes
Patients who attended group medical visits reported improvements in quality of life, as measured by the Diabetes Quality of Life Questionnaire46 (weighted mean difference −29.30, 95% CI −60.64 to 2.05); however, the results were limited to 2 RCTs and were not statistically significant.
Data on process-of-care outcomes in the RCTs were insufficient to include them in the meta-analysis. In our synthesis of findings from all 26 studies, we noted reports on aspects of patients’ engagement in their health care, including positive outcomes in the domain of self-care,21,25 physical activity,39 the setting and achievement of measurable goals,21,34,39 patient knowledge,24,31,32,41,44 self-efficacy23,25 and self-management.24,26,34,36,40,44
Interpretation
Our meta-analysis showed that group medical visits for patients with diabetes led to significant reductions in HbA1c. Small decreases have been shown to have substantial clinical impacts: a 1.0% reduction in HbA1c may be associated with a 37% decrease in microvascular complications, up to a 14% reduction in the incidence of myocardial infarction and a 21% decrease in the risk of death from diabetes.47
Patients with diabetes are known to be at increased risk of cardiovascular disease and cardiovascular-related death.48,49 Although not statistically significant, the reductions in systolic and diastolic blood pressure among patients attending group medical visits are of interest. Many lifestyle modifications such as weight reduction, dietary changes, physical activity and alcohol consumption have been found to reduce systolic blood pressure by 2–8 mm Hg.50 A reduction of 2 mm Hg in diastolic blood pressure has been associated with a 6% decrease in the risk of coronary heart disease and a 15% reduction in stroke and transient ischemic attacks.51
An additional factor to consider when caring for patients with diabetes is their quality of life. Although only 2 of the RCTs measured this outcome using the Diabetes Quality of Life Questionnaire, the aspects of patients’ quality of life examined in many of the other studies were similar to the domains covered in the questionnaire.
Only 2 of the RCTs examined the risk of hypoglycemic events associated with group medical visits.22,32 Studies have shown that intensive glucose-lowering therapy among patients with diabetes may increase the risk of morbidity and mortality owing to hypoglycemic events.52,53
Limitations
There were few long-term studies examining the effectiveness of group medical visits for diabetes care. Fifteen of the 26 studies were 12 months or less in duration, and 6 studies were up to 2 years in duration. The study with the longest duration followed patients for 5 years after the intervention. Therefore, the long-term or sustainable outcomes of group medical visits are unclear, and it is difficult to know if the outcomes were maintained for a substantial length of time after the intervention.
Another limitation was that we restricted our search to include only published studies. We realize that studies showing a lack of effect may not have been published. We also included only articles written in English or translated into English, thereby excluding 2 studies not published in English.
Many of the studies involved specific populations of patients, such as those with low incomes, those with different ethnic backgrounds and veterans. Although group medical visits may work for populations with specific characteristics, the mixed results indicate that further examination of the types of populations and types of delivery models is needed.
Conclusion
Group medical visits for patients with diabetes were found to be effective in terms of reducing HbA1c. The results of our meta-analysis, combined with the other benefits reported by patients and providers, suggest that wider implementation of group medical visits for patients with diabetes will have a positive effect on patient outcomes.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Laura Housden, doctoral candidate, led the systematic review, conducted the meta-analysis and wrote the first and subsequent drafts of the article. Sabrina Wong and Martin Dawes provided feedback, expertise and direction on the methodology and ensured the accuracy of the data extraction. Sabrina Wong contributed to the selection of articles and provided direction on the assessment of article bias. Martin Dawes assisted with the meta-analysis and sensitivity analysis. All of the authors critically revised the manuscript for important intellectual content and approved the final version submitted for publication.
Funding: No direct funding was received for this study. Laura Housden was supported by a Junior Graduate Trainee Award from the Michael Smith Foundation for Health Research, the Canadian Health Services Research Foundation/Canadian Institutes of Health Research (CHSRF/CIHR) Chair Program in Advanced Practice Nursing, and the CIHR/CHSRF Tutor–PHC (Transdisciplinary Understanding and Training on Research — Primary Health Care) training program. The sponsors had no role in the design of the study, the collection, analysis or interpretation of the data, the writing of the report or the decision to submit the article for publication.
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Effectiveness of shared medical appointments delivered in primary care for improving health outcomes in patients with long-term conditions: a systematic review of randomised controlled trials
- Effectiveness of shared medical appointments delivered in primary care for improving health outcomes in patients with long-term conditions: a systematic review of randomised controlled trials
- The Psychosocial Needs of Patients Participating in Diabetes Shared Medical Appointments
- The Psychosocial Needs of Patients Participating in Diabetes Shared Medical Appointments
- Implementing video group consultations in general practice during COVID-19: a qualitative study
- A Thoughtful Rebirth of Health Care: Lessons From the Pandemic
- Feasibility of Group Visits for Advance Care Planning Among Patients with Heart Failure and Their Caregivers
- Improving Self-Care Management in Low-Income Latinos With Type 2 Diabetes Using Peer-Led U.S. Conversation Maps: A Quality Improvement Project in a Free Clinic
- Impact of a Multidisciplinary, Endocrinologist-Led Shared Medical Appointment Model on Diabetes-Related Outcomes in an Underserved Population
- Group education for adolescents with type 1 diabetes during transition from paediatric to adult care: study protocol for a multisite, randomised controlled, superiority trial (GET-IT-T1D)
- Process evaluation of team-based care in people aged >65 years with type 2 diabetes mellitus
- Process and Systems: A systems approach to embedding group consultations in the NHS
- Obesity: Are shared medical appointments part of the answer?
- Evaluation of an Ongoing Diabetes Group Medical Visit in a Family Medicine Practice
- A Group Visit Initiative Improves Advance Care Planning Documentation among Older Adults in Primary Care
- Group clinics for young adults with diabetes in an ethnically diverse, socioeconomically deprived setting (TOGETHER study): protocol for a realist review, co-design and mixed methods, participatory evaluation of a new care model
- Effectiveness of chronic care models for the management of type 2 diabetes mellitus in Europe: a systematic review and meta-analysis
- Coproduction of healthcare service
- Exercise as medicine--the use of group medical visits to promote physical activity and treat chronic moderate depression: a preliminary 14-week pre-post study
- Group Medical Visits (GMVs) in primary care: an RCT of group-based versus individual appointments to reduce HbA1c in older people
- Shared Medical Appointments in Cancer Survivorship Care: A Review of the Literature
- Multidisciplinary Group Clinic Appointments: The Self-Management and Care of Heart Failure (SMAC-HF) Trial
More in this TOC Section
Similar Articles
Collections

